Search the hub
Showing results for tags 'Implementation'.
Found 187 results
-
Content ArticleSometimes after an incident, a system-wide change is implemented that makes work more difficult and creates new problems. This story from aviation is one such example, which contains useful lessons for responding to rare events. Steven Shorrock recounts the tale.
-
Event
Digital health and care congress 2023

Patient Safety Learning posted an event in Community Calendar
untilDigital technologies have transformed how health and care services are offered and used, and the better and more widespread use of these technologies bring further opportunities to improve people’s health and experiences of services. Through the lens of both the workforce and people who draw on health and care services, this event will explore how to successfully adopt digital solutions in health and care and the practical realities of implementation. At this event, you’ll have the opportunity to discuss different digital technologies, and hear how they can be used innovatively to improve service design and delivery and user experience, as well as help tackle the current pressures facing the NHS and the wider system. Join experts from The King’s Fund and across the health and care system to share best practice and consider how we can ensure the system has the skills, leadership and culture to harness digital transformation. Register -
Content ArticleImperial College Healthcare share a poster on their strategic goals and their values and behaviours.
-
Content ArticleThe number of patients who die from post-surgical complications in low- and middle-income countries is shockingly high. In Africa alone, more than 600,000 people die each year after surgery, mostly from causes that are relatively easy to treat. This blog by Pierre Barker, Chief Scientific Officer at the Institute for Healthcare Improvement (IHI) looks at a method for reducing post-surgical death called the '5Rs for rescue': Risk stratification Recognise deterioration Respond Reassess Reflect/Redesign He describes how the IHI will test how to support the reliable implementation of the '5Rs for Rescue', which aims to reduce mortality by 25%.
-
Content ArticleStatement from Maria Caulfield, Parliamentary Under Secretary of State (Minister for Mental Health and Women's Health Strategy) on the Government’s initial response to the report of the independent review into the maternity and neonatal services at East Kent University NHS Foundation Trust that was published on the 19 October 2022. NHS England commissioned Dr Bill Kirkup to undertake this review following concerns about the quality and outcomes of care.
-
Content ArticleThe NHS Patient Safety Incident Response Framework (PSIRF) was launched in 2022 and is intended for full implementation by Autumn 2023. PSIRF requires Integrated Care Board (ICB)’s to work collaboratively with providers to develop a Patient Safety Incident Response Plan (PSIRP) and Patient Safety Incident Response Policy. Within the PSIRP, each organisation must work with their ICB and other stakeholders to identify how it will respond proportionately to all incidents requiring investigation. Suffolk and North East Essex NHS Foundation Trust share their Standard Operating Procedure on PSIRF ICB sign off process.
-
Content ArticleThis study from Jones et al. identified wide variability in the implementation of the Guardian role and concluded that optimal implementation has six components.
-
Content ArticleJudy Walker talks about improving team performance through the After Action Review approach and the importance of AAR Conductor training.
-
Content ArticleThis download is the third of three chapters of a book which complements the Chartered Institute of Ergonomics and Human Factors' Healthcare Learning Pathway and is intended as a practical resource for students The book aims to provide well-founded, practical guidance to those responsible for leading and implementing human factors programmes and interventions in health and social care.
-
Content Article
Safety for All: 2022 Conference Report

Mark Hughes posted an article in Improving patient safety
This report provides an overview of speeches, presentations and panel sessions held at the inaugural Safety for All conference, which took place at the Royal College of Physicians in London on Wednesday 7 December 2022. It has been published by the Safety for All campaign, which calls for improvements in, and between, patient and healthcare worker safety to prevent patient safety incidents and deliver better outcomes for all. The campaign is supported by Patient Safety Learning and the Safer Healthcare and Biosafety Network. -
Content Article
 This is part of our series of Patient Safety Spotlight interviews, where we talk to people working for patient safety about their role and what motivates them. Lucy and Rebecca talk to us about their experience as Patient Safety Incident Response Framework (PSIRF) early adopters. They discuss how PSIRF puts patients at the centre of incident investigations, and the challenges and opportunities they have faced in implementing PSIRF at West Suffolk NHS Foundation Trust.
This is part of our series of Patient Safety Spotlight interviews, where we talk to people working for patient safety about their role and what motivates them. Lucy and Rebecca talk to us about their experience as Patient Safety Incident Response Framework (PSIRF) early adopters. They discuss how PSIRF puts patients at the centre of incident investigations, and the challenges and opportunities they have faced in implementing PSIRF at West Suffolk NHS Foundation Trust.- Posted
- 1 comment
-
3
-
- (and 7 more)
-
Content ArticleIntegrated care systems are now legally responsible for leading a localised approach that brings multiple aspects of the healthcare system closer together, and for working better with social care and other public services. However, this is not a new aspiration, so why should it be any different this time? The Nuffield Trust hosted a series of roundtables to discuss concerns with stakeholders and experts to try and understand how to ensure the aims are achieved. This report summarises these findings and offers ways forward as the new era gets underway.
-
Content ArticleThis article in BMJ Open Quality aimed to improve patient safety by examining the organisational and individual factors that contribute to adverse events, enabling corrective action so that errors are not repeated. Using interviews and observations of Trust meetings at a single Hospital Trust in the Midlands, England, this qualitative study: analysed whether the attitudes and behaviours of clinicians and managers are aligned with a Just Culture. identified barriers and enablers to an organisation adopting a Just Culture. The study found evidence of a fair incident management process within the Trust; however, there was no agreed vision of a Just Culture and the majority of the staff were unfamiliar with the term. Negative perspectives relating to clinical incidents and their management persist among staff with many having concerns about being the subject of an investigation and doubts about whether they drive improvement.
-
Content ArticleIn this blog, Judy Walker, an After Action Review (AAR) expert, looks at how effective learning from disasters and incidents can restore hope and trust, offering long-term improvements to systems that have failed. She talks about how public inquiries, although they can seem frustratingly slow, benefit society when the relevant authorities ensure that learning is understood and implemented. She compares this to the impact of AARs, highlighting that people’s trust in the process is linked to their perception of the changes that happen as a result of the AAR. She outlines three steps that NHS providers should take to ensure the AAR process is effective in restoring hope: Highlight to all staff on a regular basis, the benefits that are being delivered due to AARs Ensure patients and family members are provided with specific information about how AARs prevent future harms Support the people who lead AARs to do so skilfully, so that quality is assured and staff can trust in the safety and value of the process.
-
Content ArticleSafety-II is moving beyond the conceptual, with practical applications emerging from the fog of models and theory. But critics still point to a lack of evidence and limited real-world proof that the promise is justified. This blog reports on a webinar by Mark Sujan and Simon Gill that looked at how to implement Safety-II thinking in real world settings. The blog outlines different elements of the webinar including: a case study of anticipatory practice being used to reduce serious harm from falls in an emergency department a discussion on how to move towards a non-hierarchical clinical leadership challenges to adopting Safety-II principles evaluation of Safety-II: how do you measure a non-event?
-
Content Article
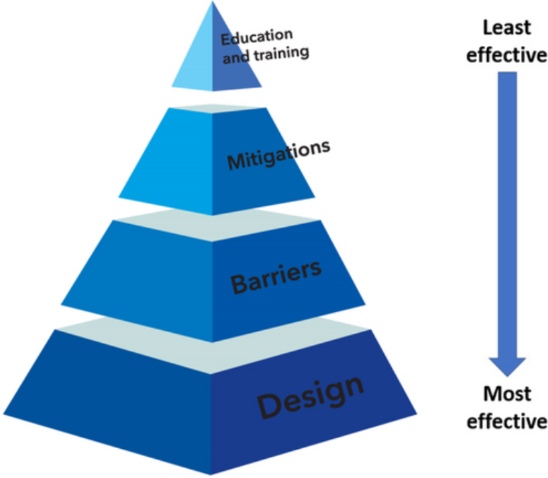 This guidance on implementing human factors in anaesthesia has been produced by the Difficult Airway Society and the Association of Anaesthetists. Human factors is an evidence-based scientific discipline used in safety critical industries to improve safety and worker wellbeing; implementing human factors strategies in anaesthesia has the potential to reduce the reliance on exceptional personal and team performance to provide safe and high-quality patient care. A three-stage Delphi process was used to formulate a set of 12 recommendations: these are described using a ‘hierarchy of controls’ model and classified into design, barriers, mitigations and education and training strategies.
This guidance on implementing human factors in anaesthesia has been produced by the Difficult Airway Society and the Association of Anaesthetists. Human factors is an evidence-based scientific discipline used in safety critical industries to improve safety and worker wellbeing; implementing human factors strategies in anaesthesia has the potential to reduce the reliance on exceptional personal and team performance to provide safe and high-quality patient care. A three-stage Delphi process was used to formulate a set of 12 recommendations: these are described using a ‘hierarchy of controls’ model and classified into design, barriers, mitigations and education and training strategies. -
Content ArticleThe Cambridge Elements series offers a comprehensive and authoritative set of overviews of different improvement approaches that can be applied to healthcare. Each publication explores the thinking behind them, examines evidence for each approach and identifies areas of debate. Publications available include: Design creativity Values and ethics Statistical process control Approaches to spread, scale-up, and sustainability Health economics Governance and leadership Workplace conditions Reducing overuse Simulation as an improvement technique Implementation science Operational research approaches Making culture change happen Co-producing and co-designing Collaboration-based approaches The positive deviance approach
-
Content ArticleRecording of the Health and Social Care Committee meeting held on Tuesday 13 December 2022. Meeting started at 10.03am, ended 11.45am.
-
Content ArticleThis policy paper, published by the Department of Health and Social Care, provides an update on the UK Government’s progress in implementing the recommendations of the Independent Medicines and Medical Devices Safety (IMMDS) Review, sometimes referred to as the Cumberlege Review.
- Posted
- 3 comments
-
- (and 6 more)
-
Content Article
 This is part of our series of Patient Safety Spotlight interviews, where we talk to people working for patient safety about their role and what motivates them. Tracey talks to us about how her love of applying psychology led to her role in patient safety, the importance of putting users at the centre of developing the Patient Safety Incident Response Framework (PSIRF), and what we can learn from magicians about patient safety.
This is part of our series of Patient Safety Spotlight interviews, where we talk to people working for patient safety about their role and what motivates them. Tracey talks to us about how her love of applying psychology led to her role in patient safety, the importance of putting users at the centre of developing the Patient Safety Incident Response Framework (PSIRF), and what we can learn from magicians about patient safety.- Posted
- 1 comment
-
- (and 5 more)
-
Content ArticleIn this episode of the What the HealthTech? podcast, Radar Healthcare's Chief Product Officer Mark Fewster speaks to Helen Hughes, Chief Executive of Patient Safety Learning. to get the lowdown on NHS England's new Patient Safety Incident Response Framework (PSIRF). Helen talks about how PSIRF is going to drive an open and just culture, what can be expected after the transition and why the implementation process is key to PSIRF's success. Listen on Spotify Listen on YouTube
-
Content ArticleIn this blog for The Patients Association, Patient Safety Commissioner Henrietta Hughes looks at the importance of patient involvement in improving patient safety. She argues that patient voices should be embedded in the design and delivery of healthcare, and highlights that services and organisations need to seek feedback from patients from a wide variety of backgrounds. She also outlines why shared decision making and consent are vital to ensure patients are safe and have more control over their care and treatment.
-
Content ArticleThis Canadian study in the Journal of Patient Safety describes an initiative that introduced system-wide changes to practice and patient safety culture in a rapid time frame. it looks at the implementation of a 'zero harm' approach to eliminate preventable harm across a wide variety of clinical areas. In less than a year, the intervention increased patient safety incident reporting by 37% while decreasing falls with injury by 39%, pressure injury rates by 37% and central line–associated blood stream infections by 34%.
-
Content ArticleThe Patient safety incident response framework (PSIRF) represents a new approach to responding to incidents. Under PSIRF, those leading the patient safety agenda within provider organisations, together with internal and external stakeholders (including patient safety partners, commissioners, NHS England, regulators, Local Healthwatch, coroners etc), decide how to respond to patient safety incidents based on the need to generate insight to inform safety improvement where it matters most. Key issues must first be identified and described as part of planning activities before an organisation agrees how it intends to respond to maximise learning and improvement. This guidance has been developed collaboratively between Stop the Pressure Programme, National Wound Care Strategy leads and members of the Patient Safety Team, with the support from the Patient Safety Incident Response Framework (PSIRF) Implementation and Working Groups.
-
Content ArticleIn this blog, Melanie Ottewill, National Investigator and Senior Investigation Science Educator at the Healthcare Safety Investigation Branch (HSIB), explains how HSIB's work is supporting the NHS to adopt a systems approach to local safety investigations through the Patient Safety Incident Response Framework (PSIRF). She looks at how PSIRF promotes a proportionate response to patient safety incidents, highlights the importance of organisations developing patient safety incident response plans and explores how PSIRF promotes compassionate involvement in patient safety incidents. She also highlights guidance to support staff in planning PSIRF implementation.




