Search the hub
Showing results for tags 'Human factors'.
Found 549 results
-
Content ArticleMusculoskeletal disorders (MSDs) are one of the main causes of ill health in the workplace, leaving many employees with painful long-term injuries. Health and social care are industries with a particularly high incidence of MSDs among staff. This infographic by the Chartered Institute for Ergonomics and Human Factors (CIEHF) lists the warning signs to be aware of and gives lots of easy-to-follow practical advice on how to prevent or reduce the risk of developing symptoms. There’s also a link to find exercises that could help prevent injuries occurring.
-
Content ArticleThe original National Safety Standards for Invasive Procedures (NatSSIPs) were published in 2015. Understanding of how to deliver safe care in a complex and pressurised system is evolving. These revised standards (NatSSIPs2) are intended to share the learning and best practice to support multidisciplinary teams and organisations to deliver safer care.
-
Content ArticleSafety-II is moving beyond the conceptual, with practical applications emerging from the fog of models and theory. But critics still point to a lack of evidence and limited real-world proof that the promise is justified. This blog reports on a webinar by Mark Sujan and Simon Gill that looked at how to implement Safety-II thinking in real world settings. The blog outlines different elements of the webinar including: a case study of anticipatory practice being used to reduce serious harm from falls in an emergency department a discussion on how to move towards a non-hierarchical clinical leadership challenges to adopting Safety-II principles evaluation of Safety-II: how do you measure a non-event?
-
Content ArticleThis webinar was organised by the Chartered Institute of Ergonomics & Human Factors (CIEHF) in partnership with the Israel Human Factors and Ergonomics Association (IHFEA). It looks at the impact of human factors in the design and use of a range of medical devices. Experts from Israel, the Netherlands and the UK share their insights about the challenges involved and how they were overcome. In her talk, Avital Zik shares examples from her experience in leading the human factors work of the Medtronic Lung Navigation system. Lung cancer care is currently invasive, ineffective, inefficient, difficult for users and often comes too late. Avital's team is on a mission is to transform the future of lung care.
-
Content Article
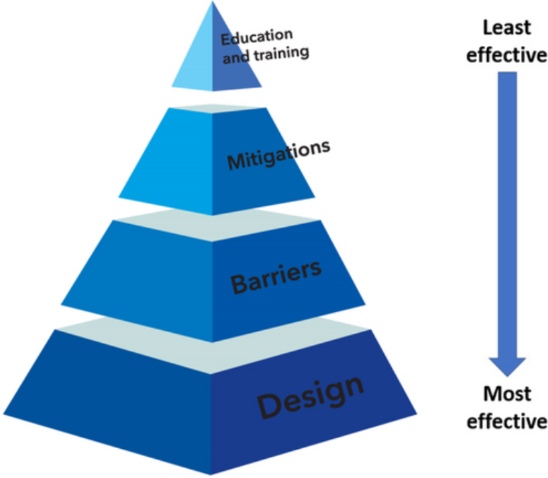 This guidance on implementing human factors in anaesthesia has been produced by the Difficult Airway Society and the Association of Anaesthetists. Human factors is an evidence-based scientific discipline used in safety critical industries to improve safety and worker wellbeing; implementing human factors strategies in anaesthesia has the potential to reduce the reliance on exceptional personal and team performance to provide safe and high-quality patient care. A three-stage Delphi process was used to formulate a set of 12 recommendations: these are described using a ‘hierarchy of controls’ model and classified into design, barriers, mitigations and education and training strategies.
This guidance on implementing human factors in anaesthesia has been produced by the Difficult Airway Society and the Association of Anaesthetists. Human factors is an evidence-based scientific discipline used in safety critical industries to improve safety and worker wellbeing; implementing human factors strategies in anaesthesia has the potential to reduce the reliance on exceptional personal and team performance to provide safe and high-quality patient care. A three-stage Delphi process was used to formulate a set of 12 recommendations: these are described using a ‘hierarchy of controls’ model and classified into design, barriers, mitigations and education and training strategies. -
Content ArticleIn this blog, published by the Healthcare Safety Investigation Branch, Laura Pickup talks about the importance of considering the design of healthcare equipment and how it impacts on risk to patient safety. She highlights that there is a confusion between ‘use error’ and ‘abnormal use’ and questions whether it is really fair to hold NHS staff accountable when the use of equipment or devices has led to a safety incident.
-
Content ArticleIn this article for The Guardian, an anonymous hospital consultant describes the situation in many NHS emergency departments in January 2023—patients ready for medical admission waiting in ambulances in the hospital car park, patients receiving IV antibiotics in chairs in the corridor and staff completely overwhelmed by the workload. The author highlights that accident and emergency departments are now being used for a purpose for which they were not designed—looking after patients who need to be admitted to hospital wards. They describe the implications of this on patient safety and staff wellbeing and argue that the NHS and Government need to call the situation what it is—a crisis—or we will come to accept poor quality care and low patient safety standards as the norm.
-
Content ArticleVideo recording and slides of a webinar presented by Mary Dixon-Woods, Professor of Medical Sociology and Wellcome Trust Investigator.
-
Content ArticleIn this article, Roger Kline, Research Fellow at Middlesex University, explains what caused the sinking of the Herald of Free Enterprise ferry. The sinking of the Herald of Free Enterprise on March 6 1987 with the loss of 198 lives was an accident waiting to happen, highlighting the devastating consequences of abandoning safe working practices in the name of financial savings. Human factors science learned from the Herald disaster is widely applied in sectors as diverse as nuclear power stations and healthcare.
-
Content ArticleRoyal Cornwall QI conference online book supporting the conference. The online brochure highlights all the quality improvement projects at Royal Cornwall Hospitals.
-
Content ArticleThis study in Plos One used a prospective error analysis method—the Systematic Human Error Reduction and Prediction Approach (SHERPA)—to examine the process of dispensing medication in community pharmacy settings and identify solutions to avoid potential errors. These solutions were categorised as strong, intermediate or weak based on an established patient safety action hierarchy tool. The authors identified 88 potential errors with a total of 35 remedial solutions proposed to avoid these errors in practice. Sixteen (46%) of these remedial measures were categorised as weak, 14 (40%) as intermediate and 5 (14%) as strong according to the Veteran Affairs National Centre for Patient Safety action hierarchy. The authors suggest that future research should examine the effectiveness of the proposed remedial solutions to improve patient safety.
-
Content ArticleHuman factors engineering or ergonomics (HFE) is a scientific discipline broadly focused on interactions among humans and other elements of a system. This article explores how HFE can be used to improve patient safety, in particular using the Systems Engineering Initiative for Patient Safety (SEIPS) model, which depicts key characteristics and interactions between three core components: work system process outcomes
-
Content ArticleThis blog is part of a series in which Steven Shorrock, an interdisciplinary humanistic, systems and design practitioner, outlines seven ‘archetypes of human work’. This blog looks specifically at 'The Messy Reality' archetype, which is characterised by adjustments, adaptations, variations, trade-offs, compromises and workarounds that are hard to prescribe and hard to identify, but that can become accepted and unremarkable for insiders. Steven examines what 'The Messy Reality' is, why it exists and highlights some examples from the aviation and healthcare industries.
-
Content Article
Did you know? Extravasation (November 2022)

Patient_Safety_Learning posted an article in Extravasation
Extravasation is the accidental leakage of any liquid from a vein into the surrounding tissues, which can cause serious harm to the patient (NHS England, 2017). From 1 April 2011 until 31 March 2021 the NHS paid £15.6 million in damages relating to extravasation. This leaflet, published by NHS Resolution, aims to share learning from those claims. -
Content ArticleThe third leading cause of death in the US is its own healthcare system—medical errors lead to as many as 440,000 preventable deaths every year. To Err Is Human is an in-depth documentary about this silent epidemic and those working quietly behind the scenes to create a new age of patient safety. Through interviews with leaders in healthcare, footage of real-world efforts leading to safer care, and one family’s compelling journey from being victims of medical error to empowerment, the film provides a unique look at the US healthcare system’s ongoing fight against preventable harm.
-
Content ArticleThis article in Time reviews the documentary film 'To Err is Human', which explores the tragic outcomes of medical errors and the medical culture that allows them to persist. The film follows the Sheridans, a family from Boise, Idaho on their journey to understand how two major medical errors befell their family: one that contributed to a case of cerebral palsy, and another that involved a delayed cancer diagnosis and ended in death.
-
Content ArticleIn this review, Jane Carthey and colleagues discuss human factors research in cardiac surgery and other medical domains. The authors describe a systems approach to understanding human factors in cardiac surgery and summarise the lessons that have been learned about critical incident and near-miss reporting in other high technology industries that are pertinent to this field.
-
Content ArticleThe Patient Safety Database (PSD), previously called the Anesthesia Safety Network, is committed in the delivery of better perioperative care. Its primary goal is to make visible the lack of reliability of healthcare and the absolute necessity to build a new system for improving patient safety. This year, PSD has also been involved in the development of the SafeTeam Academy, an e-learning training platform associated with the Patient Safety Database, which offers video immersive courses using the power of cinema to train healthcare professionals. This is the latest newsletter from PSD, featuring a wide range of content by safety experts across Europe.
-
News Article
Drug shortages linked with medication errors, study results suggest

Patient Safety Learning posted a news article in News
A French study of adverse drug reactions has a highlighted a link between drug shortages and medication error. Data from the French Pharmacovigilance Database show that medication errors were identified in 11% of the 462 cases mentioning a drug shortage. The researchers found that medication errors usually occurred at the administration step and involved a human factor. “A drug shortage may lead to a replacement of the unavailable product by an alternative,” the researchers wrote. “However, this alternative may have different packaging, labelling, dosage and sometimes a different route of administration that may increase the risk of a medication error.” Read full story (paywalled) Source: The Pharmaceutical Journal, 11 October 2022 -
Content ArticleAdherence to best practices for sepsis management at a small community hospital was below system, state and national benchmarks and affected vital indicators, including mortality. This study carried out by Megan Kiser aimed to improve sepsis best practice compliance by implementing human factors–influenced interventions.
-
Content ArticleWhether beginning a new effort or trying to keep people motivated to better prepare for future hazards, applying risk communication principles will lead to more effective results. This self-guided module introduces seven best practices, numerous techniques, and examples to help you improve your communication efforts. Please note that this training focuses on improving risk communication skills for coastal hazards planning and preparedness, however the principles can be adapted for any setting, including healthcare.
-
Content ArticleHindsight bias (colloquially known as ‘the retrospectoscope’) is the tendency to perceive past events as more predictable than they actually were. It has been shown to play a significant role in the evaluation of an past event, and has been demonstrated in both medical and judicial settings. This study in Clinical Medicine aimed to determine whether hindsight bias impacts on retrospective case note review, through an internet survey completed by doctors of different grades. The authors found that in some cases, doctors are markedly more critical of identical healthcare when a patient dies compared to when a patient survives. Hindsight bias while reviewing care when a patient survives might prevent identification of learning arising from errors. They also suggest that hindsight bias combined with a legal duty of candour will cause families to be informed that patients died because of healthcare error when this is not a fact.
-
Content ArticleThe ‘No Blame Culture’ being adopted by the NHS draws attention from individuals and towards systems in the process of understanding an error. This article in the Journal of Applied Philosophy argues for a ‘responsibility culture’, where healthcare professionals are held responsible in cases of foreseeable and avoidable errors. The authors argue that proponents of No Blame Culture often fail to distinguish between blaming someone and holding them responsible, They examine the idea of ‘responsibility without blame’, applying this to cases of error in healthcare. Sensitive to the undesirable effects of blaming healthcare professionals and to the moral significance of holding individuals accountable, the authors argue that a responsibility culture has significant advantages over a No Blame Culture as it can enhance patient safety and support medical professionals in learning from their mistakes, while also recognising and validating the legitimate sense of responsibility that many medical professionals feel following avoidable error, and motivating medical professionals to report errors.
-
Content Article
 A ‘Just Culture’ aims to improve patient safety by looking at the organisational and individual factors that contribute to incidents. It encourages people to speak up about their errors and mistakes so that action can be taken to prevent those errors from being repeated. Adam Tasker and Julia Jones are graduate medical students at Warwick Medical School. They wanted to explore doctors’ perceptions of culture and identify ways to foster a Just Culture, so they conducted a qualitative research study at one of the hospitals where they were doing their medical training. We asked them about why Just Culture is important in the health and care system, and what they discovered from their research.
A ‘Just Culture’ aims to improve patient safety by looking at the organisational and individual factors that contribute to incidents. It encourages people to speak up about their errors and mistakes so that action can be taken to prevent those errors from being repeated. Adam Tasker and Julia Jones are graduate medical students at Warwick Medical School. They wanted to explore doctors’ perceptions of culture and identify ways to foster a Just Culture, so they conducted a qualitative research study at one of the hospitals where they were doing their medical training. We asked them about why Just Culture is important in the health and care system, and what they discovered from their research. -
Content ArticleIn this 1202 Human Factors Podcast, Rob Hutton gives us an insight into naturalistic decision making and how it takes methods out of the Lab.


