Search the hub
Showing results for tags 'Recommendations'.
-
News Article
Bereaved call for body to enforce coroners’ advice

Patient Safety Learning posted a news article in News
Relatives of a teenage rape survivor who died after failures by mental health services are joining other families to demand a new body to enforce coroners’ recommendations to prevent future deaths. Campaigners claim the failure to act on hundreds of coroners’ recommendations every year, and to learn from the findings of often expensive inquiries into disasters, means the same mistakes are being repeated. Gaia Pope, 19, was diagnosed with post-traumatic stress disorder after revealing that she had been drugged and raped when she was 16. She was found dead in undergrowth on a cliff 11 days after disappearing in Swanage, Dorset, in 2017. After one of the longest inquests in legal history, the coroner, Rachael Griffin, made multiple reports last year to authorities including the NHS and police to prevent future deaths, but Pope’s family says most have not been acted upon. The Inquest campaign, which works with families bereaved by state-related deaths, is calling for a “national oversight mechanism” to collate recommendations and responses in a new national database, analyse responses from public bodies, follow up on progress and share common findings. Read full story (paywalled) Source: The Times, 27 June 2023 -
News Article
Patient safety: Each UK nation needs overarching lead, report urges
Patient Safety Learning posted a news article in News
A new patient safety chief should be appointed in each of the four UK nations to oversee health and social care and tackle the currently “fragmented and complex” system, experts have urged. The Professional Standards Authority for Health and Social Care (the body that oversees the 10 statutory bodies that regulate health and social care professionals in the UK, including the General Medical Council) has called for what it described as a radical rethink to improve safety in care. In a report published last week, it recommended the appointment of an independent health and social care safety commissioner (or equivalent) for each UK country. These commissioners would identify current and potential risks across the whole health and social care system, it said, and instigate necessary action across organisations. Read full story (paywalled) Source: BMJ, 6 September 2022 Related reading Working together to achieve safer care for all: a blog by Alan Clamp (chief executive of the Professional Standards Authority) Joining up a fragmented landscape: Reflections on the PSA report ‘Safer care for all’ (a blog from Patient Safety Learning -
News Article
Doctors warn Truss over NHS ‘fantasy’
Patient Safety Learning posted a news article in News
Liz Truss has been warned against “fantasy predictions” that the NHS can return to normal without radical change and was told that “unacceptable standards” are being normalised. In a rare political intervention, the professional standards body for the UK’s 220,000 doctors agreed that the NHS was routinely letting down patients. The Academy of Medical Royal Colleges said politicians must be prepared for radical changes to save the health service. Closing smaller hospitals, accepting that routine dentistry cannot be free for everyone and a return of Covid volunteers to allow doctors to treat more patients were all suggested by the head of the academy. The academy released a report that declared the NHS was in crisis, writing: “The system is providing increasing proportions of care or services which are sub-standard, threaten patient safety, and should not be acceptable in a country with the resources that we have in the United Kingdom. If we do not act with urgency, we risk permanently normalising the unacceptable standards we now witness daily.” The report sets out a series of recommendations for reform, including boosting staff numbers, reforming social care and spending more on technology. Helen Stokes-Lampard, the academy’s chairwoman, said patients were facing a “dismal winter” and that politicians must take difficult decisions. “If we don’t make changes it will inevitably deteriorate further,” she said. “The demand isn’t going away, the pressure isn’t going away, which is why the challenge for our government and for our whole society is to confront these issues and have a difficult conversation.” Read full story (paywalled) Source: The Times, 9 September 2022 -
News Article
Breast surgeon's victim wants faster improvements
Patient Safety Learning posted a news article in News
Victims of breast surgeon Ian Paterson said independent inquiry improvements are not being implemented fast enough. Paterson was jailed in 2017 after he was found to have carried out needless operations on patients across Birmingham and Solihull. The 2020 report's recommendations include the recall of his 11,000 patients to assess their treatment. The Department of Health and Social Care (DHSC) said it is working to stop future patients facing similar harm. On Sunday, ITV screened a documentary 'Bodies of Evidence: The Butcher Surgeon' which featured victim and campaigner Debbie Douglas, who was instrumental in getting the inquiry established. She said the government needs "to put pace behind" the work to implement the 15 recommendations it made. "It is important those recommendations are embedded in legislation, it is important there is governance over those recommendations to stop another Paterson, it is important that there is a proper consent procedure," she said. The recommendations called for consultants to write directly to patients to explain proposed surgical treatment as standard practice, a public register to detail which types of operations surgeons are able to perform and for patients to be given time to reflect on their diagnosis and treatment options before they are asked to consent to surgery. Read full story Source: BBC News, 14 June 2022 -
News Article
Failure to achieve mental health pledge in England ‘inhumane’, say psychiatrists
Patient Safety Learning posted a news article in News
Adult mental health patients in England have spent more than 200,000 days being treated in “inappropriate” out-of-area placements – at a cost to the NHS of £102m – in the year since the government pledged to end the practice. The Royal College of Psychiatrists, which carried out the analysis, says such placements, in which mental health patients can be sent hundreds of miles from home, are a shameful and dangerous practice that must stop. The government said it would end such placements by April last year but, in the 12 months since, 205,990 days were spent inappropriately out of area, at a cost equivalent to the annual salaries of more than 900 consultant psychiatrists, the college found. Dr Adrian James, the college’s president, said: “The failure to eliminate inappropriate out-of-area placements is a scandal. It is inhumane and is costing the NHS millions of pounds each year that could be spent helping patients get better. “No one with a mental illness should have to travel hundreds of miles away from home to get the treatment they desperately need.” He said investment was needed in local, properly staffed beds, alternatives to admission, and follow-up care in the community as well as government backing “to address the workforce crisis that continues to plague mental health services”. Read full story Source: The Guardian, 13 June 2022 -
News Article
Ministers blasted by scandal inquiry chair
Patient Safety Learning posted a news article in News
The government’s response to the East Kent maternity scandal inquiry has been condemned as ‘very disappointing’ by its chair. More than four months on from the inquiry report, ministers this morning issued what they called an “initial response” to it, as a brief written statement to Parliament. It contained few specific proposals, instead saying government was kicking off a series of other reviews, and “working” with various other agencies. Inquiry chair Bill Kirkup, the well-regarded former medic and expert in care failures, told HSJ the response was poor and should have been “wider and deeper”. Dr Kirkup said the response showed government had “not grasped how fundamental” some of the issues outlined in his report were, and “what sort of initiative” was needed to address them. Read full story (paywalled) Source: HSJ, 7 March 2023 -
News Article
Eating disorder patients ‘repeatedly failed’, says England watchdog
Patient Safety Learning posted a news article in News
Urgent action is needed to prevent people dying from eating disorders, the parliamentary and health service ombudsman for England has warned, as he said those affected are being “repeatedly failed”. The NHS needs a “complete culture change” in how it approaches the condition, while ministers must make it a “key priority”, according to Rob Behrens. Little progress has been made since the publication of a devastating report by his office in 2017, which highlighted “serious failings” in eating disorder services, he said. Lives continue to be lost because of “the lack of parity between child and adult services”, and “poor coordination” between NHS staff involved in treating patients. There remain issues with the training of medical professionals, Behrens added. “We raised concerns six years ago in our ignoring the alarms report, so it’s extremely disappointing to see the same issues still occurring,” he said. “Small steps in improvements have been taken, but progress has been slow, and we need to see a much bigger shift in the way eating disorder services are delivered." Read full story Source: The Guardian, 27 February 2023 -
News Article
Derby maternity deaths may have been prevented
Patient Safety Learning posted a news article in News
Three women who died under the care of a hospital's maternity unit may have survived if earlier recommendations had been implemented, a report has said. The cases occurred at University Hospitals of Derby and Burton (UHDB) NHS Foundation Trust over 16 months. A review by the Healthcare Safety Investigation Branch (HSIB) also found a culture of intimidation and bullying. The report found that although there was no common theme to the deaths - and four other life-threatening cases that occurred in the same period - processes and leadership had been inconsistent and fragmented. HSIB said "robust action planning and prompt addressing of the learning" from previous recommendations from other investigations "may have had an impact on the outcome for the women who received care during the seven events included in this thematic review". Read full story Source: BBC News, 22 February 2023 -
News Article
Millions with mental health needs not seeking NHS help, watchdog says
Patient Safety Learning posted a news article in News
Millions of people in England with mental ill-health are not seeking NHS help, and many who get it face long delays and a “poor experience”, a report says. Long waits for care will persist for years because soaring demand, exacerbated by Covid, will continue to outstrip the ability of severely understaffed mental health services to provide speedy treatment, the National Audit Office (NAO) found. The report found that “NHS mental health services are under continued and increasing pressure and many people using services are reporting poor experiences”. Under-18s, the LGBT+ community, minority ethnic groups and people with more complex needs are most likely to find the system inadequate. “While funding and the workforce for mental health services have increased and more people have been treated, many people still cannot access services or have lengthy waits for treatment,” the NAO said. It found: An estimated 8 million people with mental health needs are not in contact with NHS services. There are 1.2 million people waiting for help from community-based mental health services. While the mental health workforce grew by 22% between 2016-17 and 2021-22, the NHS recorded a 44% increase in referrals over the same period. In 2021-22, 13% of mental health staff quit. Read full story Source: The Guardian, 9 February 2023 -
News Article
Players told to 'sit it out' under new concussion guidance
Patient Safety Learning posted a news article in News
Anyone with suspected concussion must be immediately removed from football, rugby and other sports and rest for at least 24 hours, under new guidance for grassroots clubs. It says the NHS 111 help-line should be called and players should not return to competitive sport for at least 21 days. The UK-wide guidelines are aimed at parents, coaches, referees and players. Its authors say a "culture change" in the way head injuries are dealt with is needed. "We know that exercise is good for both mental and physical health, so we don't want to put people off sport," Prof James Calder, the surgeon who led the work for the government, said. "But we need to recognise that if you've got a head injury, it must be managed and you need to be protected, so that it doesn't get worse." Read full story Source: BBC News, 2 May 2023 -
Content ArticleSedation for therapeutic and investigative procedures in healthcare is extensively and increasingly used. In 2013 the Academy of Medical Royal Colleges (the Academy) published Safe sedation practice for healthcare procedures: Standards and guidance (this updated and replaced earlier guidance). The guidance recommended core knowledge, skills and competencies required for the safe delivery of effective sedation. It also highlighted that safety will be enhanced by the provision of achievable standards, along with the availability of appropriate facilities and monitoring used under good organisational governance of staffing, equipment, education and practice. However, despite this, avoidable morbidity and mortality continue to occur. Service reviews by the Royal College of Anaesthetists’ (RCoA’s) Anaesthesia Clinical Services Accreditation (ACSA) programme suggest that the recommendations in the 2013 guidance have not been fully acted upon by many hospitals. Therefore, this update summarises the recommendations to provide regulators with a set of standards against which to inspect facilities providing sedation and to ensure that safety standards are being met.
-
Content ArticleTen years ago today, a public inquiry concluded that patients were subject to shocking levels of neglect at Stafford Hospital - putting it among the worst care scandals in NHS history. A young local reporter, Shaun Lintern – now The Sunday Times' health editor – helped expose the scandal. With the NHS again under huge pressure, can we be sure the same failings won't happen again? In this podcast, part of the Stories of our Times podcast series, Shaun speaks to the barrister who chaired the inquiry.
-
Content ArticleLast year, the independent NHS Race and Health Observatory commissioned consultancy, Public Digital, to undertake a ‘digital discovery’ project to explore the lived experience of people undergoing acute emergency hospital admissions for sickle cell and managing crisis episodes at home. The NHS Race and Health Observatory’s January 2023 publication – ‘Sickle cell digital discovery report – Designing better acute painful sickle cell care’ – sets out to understand the broad availability of digital products and services that currently exist. The report explores the range of technology that is in place for Accident and Emergency clinicians, red-cell specialists, and ambulance care, to aid timely support to sufferers on their emergency hospital arrival. A number of focus groups and interviews were carried out with those that have lived experience of the disease, including patients who have suffered acute, painful sickle cell episodes during NHS A&E admissions. Research found a lack of individual care plans in place and, more broadly, no clear definition of what constitutes an actual care plan. A number of recommendations are set out in the report for the NHS and the wider healthcare system.
-
Content Article
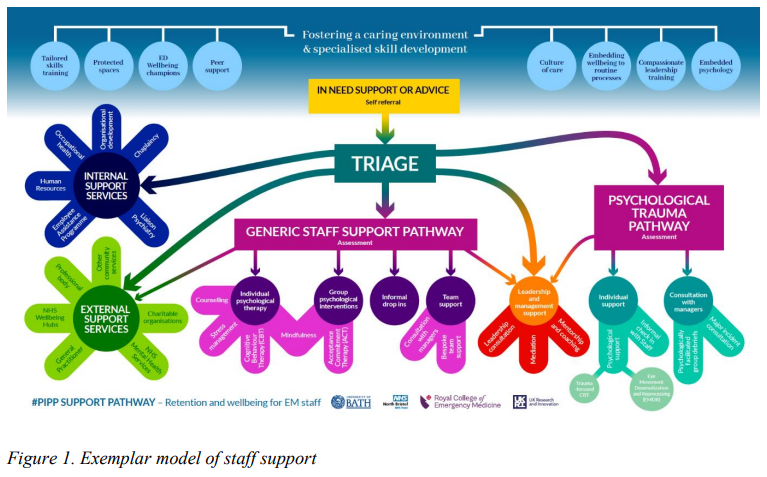 The Psychologically informed policy and practice development (PIPP) project investigated current workplace concerns, barriers to change and opportunities for development and growth, and was a collaborative project run by the Royal College of Emergency Medicine, UK Research and Innovation and the University of Bath. This document details specific evidence-based recommendations relating to four key areas identified as prioritised targets in emergency care workforce development: An environment to thrive in Cultivating a better culture A tailored pathway of care Enhanced leadership The recommendations are detailed, supported by evidence, existing guidelines and new empirical data, and are specific to the needs of the emergency care specialty.
The Psychologically informed policy and practice development (PIPP) project investigated current workplace concerns, barriers to change and opportunities for development and growth, and was a collaborative project run by the Royal College of Emergency Medicine, UK Research and Innovation and the University of Bath. This document details specific evidence-based recommendations relating to four key areas identified as prioritised targets in emergency care workforce development: An environment to thrive in Cultivating a better culture A tailored pathway of care Enhanced leadership The recommendations are detailed, supported by evidence, existing guidelines and new empirical data, and are specific to the needs of the emergency care specialty. -
Content ArticleThe Health and Social Care Select Committee have published a new report reviewing the progress that the UK Government has made in implementing the recommendations of the Independent Medicines and Medical Devices Safety Review, sometimes referred to as the Cumberlege Review. This blog sets out Patient Safety Learning’s reflections on this report.
-
Content ArticleThis Health and Social Care Select Committee report reviews the progress that the UK Government has made in implementing the recommendations of the Independent Medicines and Medical Devices Safety Review, sometimes referred to as the Cumberlege Review. You can read Patient Safety Learning’s reflections on this report here.
-
Content ArticleIn this blog, Judy Walker, an After Action Review (AAR) expert, looks at how effective learning from disasters and incidents can restore hope and trust, offering long-term improvements to systems that have failed. She talks about how public inquiries, although they can seem frustratingly slow, benefit society when the relevant authorities ensure that learning is understood and implemented. She compares this to the impact of AARs, highlighting that people’s trust in the process is linked to their perception of the changes that happen as a result of the AAR. She outlines three steps that NHS providers should take to ensure the AAR process is effective in restoring hope: Highlight to all staff on a regular basis, the benefits that are being delivered due to AARs Ensure patients and family members are provided with specific information about how AARs prevent future harms Support the people who lead AARs to do so skilfully, so that quality is assured and staff can trust in the safety and value of the process.
-
Content ArticleRecording of the Health and Social Care Committee meeting held on Tuesday 13 December 2022. Meeting started at 10.03am, ended 11.45am.
-
Content ArticleIn the UK, the focus of osteoporosis care in the NHS has been on people who have sustained a fragility fracture as a result of their underlying condition. Not much has been done to try and prevent the first fracture by promoting good bone health and proactively identifying people at higher risk. This report by the APPG on Osteoporosis and Bone Health presents the results of its inquiry into primary care provision for people with osteoporosis and those at high risk of fracture, launched in March 2022. The inquiry aimed to establish the current quality of care being offered to patients.
-
Content ArticleThis cross-sectional study in BMJ Evidence-Based Medicine aimed to understand the relationship between financial conflicts of interest and recommendations for atrial fibrillation (AF) screening in the UK. The authors looked at whether the UK media recommend for or against screening for AF and the financial conflicts of interests of AF screening commentators. The authors found that the vast majority of UK media promotes screening for AF, in contrast to the position of the independent UK National Screening Committee, which recommends against screening. Most commentators, internal NHS organisations and UK charities promoting screening had a direct or indirect financial conflict of interest. Independent information was rare and the reasons for this are unknown. They recommend readers consider the potential impact of financial conflicts on recommendations to screen.
-
Content ArticleThis policy paper, published by the Department of Health and Social Care, provides an update on the UK Government’s progress in implementing the recommendations of the Independent Medicines and Medical Devices Safety (IMMDS) Review, sometimes referred to as the Cumberlege Review.
- Posted
- 3 comments
-
- (and 6 more)
-
Content ArticleAn expert review of the clinical records of 44 deceased patients who had been under the care of neurologist Dr Michael Watt has found there were “significant failures” in their treatment and care. Dr Watt, a former Belfast Health and Social Care Trust consultant neurologist, was at the centre of Northern Ireland’s largest ever recall of patients, which began in 2018, after concerns were raised about his clinical work. More than 4,000 of his former patients attended recall appointments. At the direction of the Department of Health, in August 2021, the Regulation and Quality Improvement Authority (RQIA) commissioned the Royal College of Physicians to undertake an expert review of the clinical records of certain deceased patients who had been under the care of Dr Watt, with the intention to understand his clinical practice, to ensure learning for others and to help make care better and safer in the future.
-
Content ArticleKeeping patients safe during their care and treatment should be at the heart of any health system, including the NHS. Yet avoidable harm still occurs every day, around the world. There have been major efforts to prioritise patient safety in England, but the pandemic has shone a light on areas of care where progress has stalled, or safety has deteriorated. This report by Imperial College London's Institute of Global Health Innovation, commissioned by Patient Safety Watch, brings together publicly available data to present a national picture of patient safety in England.
- Posted
- 1 comment
-
- (and 9 more)
-
News Article
East Kent NHS inquiry finds better care might have prevented 45 babies’ deaths
Patient Safety Learning posted a news article in News
The deaths of at least 45 babies could have been avoided if nationally recognised standards of care had been provided at one of England’s largest NHS trusts, a damning inquiry has found. Dr Bill Kirkup, the chair of the independent inquiry into maternity at East Kent hospitals university NHS foundation trust, said his panel had heard “harrowing” accounts from families of receiving “suboptimal” care, with mothers ignored by staff and shut out from discussions about their own care. The inquiry’s report said: “An overriding theme, raised with us time and time again, is the failure of the trust’s staff to take notice of women when they raised concerns, when they questioned their care, and when they challenged the decisions that were made about their care.” Of 202 cases reviewed by the experts, the outcome could have been different in 97 cases, the inquiry found. In 69 of these 97 cases, it is predicted the outcome should reasonably have been different and it could have been different in a further 28 cases. Of the 65 babies’ deaths examined, 45 could have had a different outcome if nationally recognised standards of care had been provided. In nearly half of all cases examined by the panel, good care could have led to a different outcome for the families. Some of the bereaved parents accused the trust of “victim blaming” mothers for their children’s deaths. Kelli Rudolph and Dunstan Lowe, whose daughter Celandine died at five days old, said: “Doctors sought to blame Kelli for Celandine’s death. This victim blaming was the first in a long line of interactions with those in the trust who sought to delay, deflect and deny our search for the truth about what happened to our baby. “In isolation, these tactics traumatised us after the tragedy of our daughter’s death. But when seen in the light of 10 years of failures, they signal a concerted effort to cover up the trust’s responsibility for what happened to Celandine and the many others who lost their lives due to failures in clinical judgment.” Read full story Source: The Guardian. 19 October 2022 -
News ArticleA key national policy change recommended by the inquest which led to the East Kent maternity inquiry will not be implemented until next February – more than three years after it was called for by a coroner. The recommendation – that obstetric locum doctors be required to demonstrate more experience before working – was made in a prevention of future deaths report following the inquest into the death of seven-day-old Harry Richford at East Kent Hospitals University Foundation Trust. The remaining 18 recommendations from the PFD report were requiring specific actions by the trust, rather than national policy makers. The trust says they have been implemented. However, NHS England and the Royal College of Obstetricians and Gynaecologists have only in recent months produced guidance on using short-term locums in these services, and it will not come into effect until February. When it does, it will require them to complete a certification of eligibility, demonstrating they have had recent experience in a number of clinical situations, including complex Caesarean sections. Middle-grade locums have until next February to gain the certificate. The independent inquiry into maternity at the trust – prompted by Harry’s death – will report tomorrrow, Wednesday 19 October, and is expected to be highly critical of the trust, and of national efforts to make services safe over recent years. Read full story (paywalled) Source: 18 October 2022


