Search the hub
Showing results for tags 'Psychological safety'.
-
Content Article
Vicarious trauma: The invisible epidemic

Patient Safety Learning posted an article in Staff safety
 In healthcare, an insidious epidemic lurks beneath the surface, affecting the very individuals tasked with providing care: vicarious trauma by empathy. Despite its profound impact, this phenomenon remains largely unrecognised and under-discussed within the sector. As leaders, it is imperative that we shed light on this invisible trauma and acknowledge it as one of the greatest challenges facing our industry, as Margarida Pacheco explains in her blog.
In healthcare, an insidious epidemic lurks beneath the surface, affecting the very individuals tasked with providing care: vicarious trauma by empathy. Despite its profound impact, this phenomenon remains largely unrecognised and under-discussed within the sector. As leaders, it is imperative that we shed light on this invisible trauma and acknowledge it as one of the greatest challenges facing our industry, as Margarida Pacheco explains in her blog. -
Content Article
Surgical doctors needed for psychological safety research

Patient_Safety_Learning posted an article in Culture
 Are you a surgical doctor working in the NHS? Could you spare 1 hour of your time to share your insights and help researchers explore psychological safety? Shinal Patel-Thakkar, a trainee Clinical Psychologist, is seeking participants for a qualitative research study into psychological safety in surgical environments. In this interview she tells us more about the study, how people can register their interest, and provides reassurance that confidentiality will be maintained.
Are you a surgical doctor working in the NHS? Could you spare 1 hour of your time to share your insights and help researchers explore psychological safety? Shinal Patel-Thakkar, a trainee Clinical Psychologist, is seeking participants for a qualitative research study into psychological safety in surgical environments. In this interview she tells us more about the study, how people can register their interest, and provides reassurance that confidentiality will be maintained. -
Content ArticleSafety leader Helen Macfie describes why she appreciates that Safer Together: A National Action Plan to Advance Patient Safety includes workforce safety as one of its foundational areas.
-
Content Article
To coach or not to coach? Part 3 – by Dawn Stott

Dawn Stott posted an article in Good practice
 In a new series of blogs, Dawn Stott, Business Consultant and former CEO of the Association for Perioperative Practice (AfPP), discusses how coaching and developing teams can support patient safety and its outcomes. In part one and part two, Dawn looked at the strategies and coaching methodologies that can be used to develop individuals and to support patient safety, and discusses the indicators of improvement, prosocial behaviours and the importance of good communication to improve culture and, ultimately, patient safety. In the final blog of the series, Dawn discusses the importance of reflective practice and how it encourages learning and growth, and helps us to identify and address challenges.
In a new series of blogs, Dawn Stott, Business Consultant and former CEO of the Association for Perioperative Practice (AfPP), discusses how coaching and developing teams can support patient safety and its outcomes. In part one and part two, Dawn looked at the strategies and coaching methodologies that can be used to develop individuals and to support patient safety, and discusses the indicators of improvement, prosocial behaviours and the importance of good communication to improve culture and, ultimately, patient safety. In the final blog of the series, Dawn discusses the importance of reflective practice and how it encourages learning and growth, and helps us to identify and address challenges. -
Content Article
Psychological safety newsletter
Patient Safety Learning posted an article in Suggest a useful website
Each week this newsletter contains new, useful, insightful or controversial content all about psychological safety research, applications, practice and opportunities to collaborate. -
News Article
Waiting times focus ‘overshadows misconduct’, finds NHSE review
Patient Safety Learning posted a news article in News
Ambulance trusts have often prioritised capacity and response times over dealing with cases of misconduct, a review of culture in the sector for NHS England has found. The review says ambulance trusts need to “establish clear standards and procedures to address misconduct”. The work was carried out by Siobhan Melia, who is Sussex Community Healthcare Trust CEO, and was seconded to be South East Coast Ambulance Service Foundation Trust interim chief from summer 2022 to spring last year. Her report says bullying and harassment – including sexual harassment – are “deeply rooted” in ambulance trusts, and made worse by organisational and psychological barriers, with inconsistencies in holding offenders to account and a failure to tackle repeat offenders. She says “cultural assessments” of three trusts by NHSE had found “competing pressures often lead to poor behaviours, with capacity prioritisation overshadowing misconduct management”, adding: “Staff shortages and limited opportunities for development mean that any work beyond direct clinical care is seen as a luxury or is rushed. “Despite this, there is a clear link between positive organisational culture and improved patient outcomes. However, trusts often focus on meeting response time standards for urgent calls, whilst sidelining training, professional development, and research.” Read full story (paywalled) Source: HSJ, 15 February 2024 -
Content ArticleThis animation was created to highlight the specific issues for people with learning disabilities in relation to psychological trauma.
-
Content ArticleThe framework has been produced to guide organisations providing residential or supported living accommodation to adults with a learning disability who may have been impacted by a trauma history. Whilst it can be difficult to assess the impact of trauma for many people with a learning disability, particularly those with a more severe/profound learning disability, it is important to recognise the possibility of the impact of psychological trauma. Providing care practices that are trauma informed, person-centred and growth promoting are less likely to be re-traumatizing for those already exposed to trauma.
-
Content ArticleAfter an extreme traumatic event there are things that you can do to help yourself, and your colleagues, to move on. Fiona Day, medical and public health leadership coach and chartered coaching psychologist, Stacey Killick, consultant paediatrician at Glan Clwyd Hospital, and Lucy Easthope, professor in practice at Durham University’s Institute of Hazard, Risk, and Resilience and adviser on disaster recovery give their tips in this BMJ article.
-
Content ArticleA second victim is a healthcare worker who is traumatised by an unexpected adverse patient case, therapeutic mistake, or patient-associated injury that has not been anticipated. Often, the second victim experiences direct guilt for the harm caused to the patients. Healthcare organisations are often unaware of the emotional toll that adverse events can have on healthcare providers (HCPs) who can be harmed by the same incidents that harm their patients. This study aims to examine the second victim phenomenon among healthcare providers at Al-Ahsa hospitals, its prevalence, symptoms, associated factors, and support strategies.
-
EventISO 45003:2021(E) is a guidance document that provides practical advice on managing psychosocial risks in the workplace. This document is designed to help organisations prevent work-related injury and ill health of their workers and other interested parties, and to promote well-being at work. This masterclass will explore the key concepts of ISO 45003:2021(E) and how they apply specifically to healthcare settings. It will discuss strategies for identifying and assessing psychosocial risks, implementing preventive measures, monitoring effectiveness, and promoting well-being in the workplace. The goal is for you to leave this masterclass with a comprehensive understanding of how ISO 45003:2021(E) can be used to manage psychosocial risks in your own organization. You will also have an opportunity to share best practices with colleagues from other healthcare organisations. Who should attend: Clinical staff, Managers, Admin staff, Policy makers and Board members. Key learning objectives: Participants will have a comprehensive understanding of psychosocial risks in the healthcare workplace. Participants will be able to identify preventive measures that can be implemented to manage these risks. Participants will understand the importance of monitoring and evaluating the effectiveness of these measures. Participants will have an increased awareness of their own well-being and safety in the workplace. Participants will have an opportunity to share best practices with colleagues from other healthcare organisations. Register
-
Content Article
Bad management (Psychological Safety, 6 October 2023)
Patient_Safety_Learning posted an article in Staff safety
In this issue of Psychological Safety, Tom Geraghty, shares some stories of “bad” management that newsletter readers have shared with him, so we can all learn from them. A selection of the stories, chosen because they highlight key themes. Geraghty highlights the importance of self reflection and learning from our own mistakes in order to improve. Also noting that when we share our mistakes and what we’ve learned from them, the potential for learning extends beyond ourselves to everyone around us. -
Content ArticleChanges of all kinds can have a profound effect on us, both in terms of our wellbeing and performance. David Murphy has worked therapeutically with people, including front-line professionals, for over 20 years, helping them to change, and adapt to change. David talks to Steven Shorrock about dealing with traumatic events and more mundane changes.
-
Content ArticleOn 29 September 2023, a group of NHS staff and Experts by Experience joined a Teams meeting to help the National Patient Safety team in NHS England (NHSE) to answer two important questions. 1. Is it a good idea to keep asking NHS staff to record the level of psychological harm experienced by patients and service users, after a patient safety incident? 2. If so, how we can help make sure this is done as well and accurately as possible? Here is the write up of the workshop.
-
News Article
University Hospitals Birmingham: Half of staff felt bullied
Patient Safety Learning posted a news article in News
More than half of staff at a hospital trust that has been under fire for its "toxic culture" have said they felt bullied or harassed. The findings come from an independent review commissioned by University Hospitals Birmingham (UHB) NHS Trust. It has been at the centre of NHS scrutiny after a culture of fear was uncovered in a BBC Newsnight investigation. UHB has apologised for "unacceptable behaviours". It added it was committed to changing the working environment. Of 2,884 respondents to a staff survey, 53% said they had felt bullied or harassed at work, while only 16% believed their concerns would be taken up by their employer. Many said they were fearful to complain "as they believed it could worsen the situation," the review team found. Read full story Source: BBC News, 27 September 2023 -
Content ArticleThe Culture Review report was published following an independent external review of the organisational culture at University Hospitals Birmingham Trust. The external review was carried out by consultancy firm The Value Circle following a series of investigations into problems at University Hospitals Birmingham Foundation Trust over the last year.
-
Content ArticleAs awareness of the importance of psychological safety in the workplace increases, there is a corresponding increase in the number of psychometric tools, applications and services that attempt to measure psychological safety. This post on the blog Psychological Safety outlines some helpful principles for organisations to apply when choosing a psychometric tool. It lays out the following key principles, stating that in choosing a psychometric tool, we should ensure that we understand the methods and algorithms the tool uses. it’s usable and accessible for everyone. it’s secure. people retain ownership of their own data. the questions and statements actually correlate with psychological safety. it doesn’t make assumptions based upon majority culture. the tool doesn’t create perverse incentives.
-
News Article
York eating disorder clinic served unsafe food
Patient Safety Learning posted a news article in News
A hospital for adults with eating disorders has been rated inadequate after inspectors found the provision of food was "unsafe and unacceptable". A Care Quality Commission (CQC) report of the Schoen Clinic in York said some patients were given mouldy bread and one was served food containing plastic. Concerns were also raised around lack of staff and patient safety, though wards were clean and well-equipped. Schoen Clinic Group said issues raised in the report "were quickly addressed". Following the inspection in January the hospital has been placed in special measures and will be visited again in six months. Brian Cranna, CQC's head of hospital inspection, said: "The standards of care we found at Schoen Clinic York were putting patients at risk and so we have taken urgent enforcement action, which means the service must improve if it's to retain its registration." According to the report patients were put at risk of "physical and psychological harm due to unsafe and unacceptable food provision". Read full story Source: BBC News, 21 April 2022 -
News Article
Children’s services rated ‘inadequate’ as trust remains ‘outstanding’
Patient Safety Learning posted a news article in News
The children’s inpatient unit at an ‘outstanding’ mental health trust has been downgraded to ‘inadequate’ by the Care Quality Commission (CQC), amid a surge in demand for its services. The CQC previously rated child and adolescent mental health wards at Hertfordshire Partnership University Foundation Trust as “outstanding” in May 2019. But after an inspection in November and December 2021, these services were downgraded to “inadequate” overall and for the key categories of safety and leadership. Although inspecting a core service, the CQC said its visit was “not wide-ranging enough” to update overall trust ratings, so HPFT remains “outstanding” overall. Teenagers aged from 13 to 18 and admitted to Forest House, a 16-bed unit in Radlett providing HPFT’s only inpatient service for children and adolescents, told CQC inspectors they felt “unsafe”, dissatisfied with their care, and had experienced bullying by fellow patients. Leadership in the service had “significantly deteriorated” since previous inspections, CQC chiefs wrote in a report published today, and this was having a “knock-on effect in all areas of care being provided”. Staff morale was low and access to clinical psychologists limited, with a reduced ability to provide therapeutic interventions, inspectors added. Read full story (paywalled) Source: HSJ, 30 March 2022 -
News Article
Nurses’ well-being: ‘burnout’ too gentle a term for mental distress
Patient Safety Learning posted a news article in News
Burnout is not a strong enough term to describe the severe mental distress nurses and other NHS staff are experiencing, says a doctor who has led efforts to improve care for health professionals. Medical director of the NHS Practitioner Health service Dame Clare Gerada told MPs radical action was needed to improve the mental well-being of NHS staff. She said nurses and other healthcare staff should be entitled to one hour of paid reflective time per month to be written into NHS employees’ contracts, alongside mentoring, careers advice and leadership training built in throughout people’s careers. Dr Gerada was among senior clinicians who gave evidence this week to the Health and Social Care Committee, which is looking at issues around recruitment and retention of staff. She told the committee the term ‘burnout’ simply did not cover the level of stress and mental anguish experienced by NHS workers. ‘Burnout is too gentle a term for the mental distress that is going on amongst our workforce,’ she said. High suicide rates among nurses and doctors, high levels of bullying and staff being sacked because they have long-COVID are all signs the health service is failing to look after its employees, she said. ‘The symptoms we have got are the symptoms of an organisation that is unable to care for its workforce in the way that it should be caring,’ she said. Read full story Source: Nursing Standard, 25 March 2022 -
News Article
I worry we're killing people - ambulance dispatcher

Patient-Safety-Learning posted a news article in News
Ambulance staff will take part in their second day of strike action this winter on Wednesday 11 January. Alongside paramedics, call-centre staff will walk out across England and Wales in the dispute over pay. These workers play a vital role, taking calls from the public and assigning ambulance crews. An ambulance dispatcher at the North West Ambulance Service, who wishes to stay anonymous, has described working amid the extreme pressures of this winter. They said, "The thought of going in and having to manage those calls just fills me with absolute dread. I have seen people leave the ambulance service - they have had enough. We are physically and mentally exhausted." Most frustrating, the dispatcher says, is the number of crews stuck outside hospital waiting to hand patients over to accident-and-emergency staff. In the last week of 2022, more than 40% of crews in England had waits of more than 30 minutes - it should take 15. Read full story Source: BBC News, 10 January 2023 -
News Article
Staff mental health support faces axe after national funding cut
Patient Safety Learning posted a news article in News
Mental health and wellbeing hubs for NHS and social care staff could be axed within months, as national funding for them is likely to be cut, HSJ has learned. NHS England and the Department of Health and Social Care are understood to be close to ending ring-fenced national funding for the 41 hubs, which were set up in February 2021, at the peak of acute covid pressures and concern about the impact on staff. Sources told HSJ discussions were ongoing, but that it is likely integrated care systems would need to find funding themselves if they are to continue. Amid tight local finances, it is expected many will be wound down or closed. This is despite problems with low staff morale, high absence rates and with large numbers of experienced staff thought to be leaving the service. Read full story (paywalled) Source: HSJ, 4 January 2022 -
News Article
Trust top team was ‘least cohesive I’ve ever joined’, says new CEO
Patient Safety Learning posted a news article in News
A review into how a reporting error came about has uncovered tension among an ambulance trust’s previous senior leaders, including that its new CEO felt it was ‘the least cohesive team I have ever joined’. Management consultancy Verita was commissioned by London Ambulance Service Trust to carry out a review of how it came to be misreporting category 1 (the most serious) response times. The report, published in board papers on Thursday, said it was caused by a contractor’s programming error going unnoticed and concluded it was “impossible to typify the events of August 2020 as other than an avoidable failure of governance and process”. Daniel Elkeles, who joined the trust as CEO in August 2021, told the review that when he joined the senior team it was “the least cohesive team I have ever joined” and said the organisation was not “psychologically safe” for those who wanted to speak up. Read full story (paywalled) Source: HSJ, 26 May 2023 -
Content Article
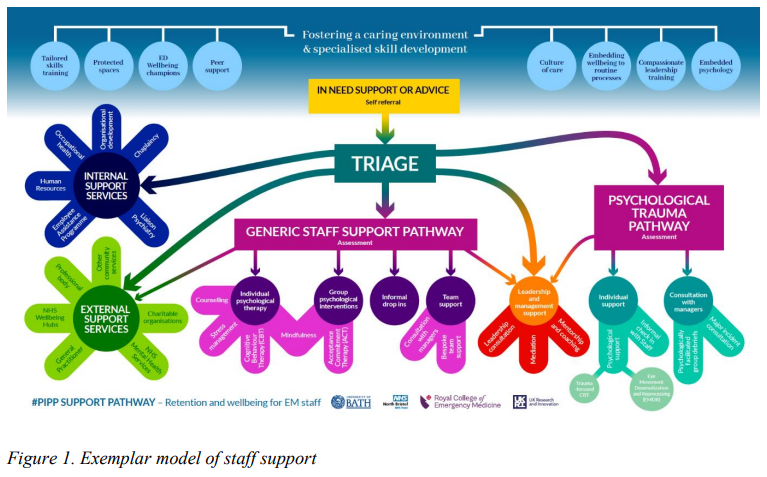 The Psychologically informed policy and practice development (PIPP) project investigated current workplace concerns, barriers to change and opportunities for development and growth, and was a collaborative project run by the Royal College of Emergency Medicine, UK Research and Innovation and the University of Bath. This document details specific evidence-based recommendations relating to four key areas identified as prioritised targets in emergency care workforce development: An environment to thrive in Cultivating a better culture A tailored pathway of care Enhanced leadership The recommendations are detailed, supported by evidence, existing guidelines and new empirical data, and are specific to the needs of the emergency care specialty.
The Psychologically informed policy and practice development (PIPP) project investigated current workplace concerns, barriers to change and opportunities for development and growth, and was a collaborative project run by the Royal College of Emergency Medicine, UK Research and Innovation and the University of Bath. This document details specific evidence-based recommendations relating to four key areas identified as prioritised targets in emergency care workforce development: An environment to thrive in Cultivating a better culture A tailored pathway of care Enhanced leadership The recommendations are detailed, supported by evidence, existing guidelines and new empirical data, and are specific to the needs of the emergency care specialty. -
Content ArticleHow can leaders move from understanding to taking actions? Listen to the Dementia UK podcast on moral injury in nursing.




