Search the hub
Showing results for tags 'Recommendations'.
Found 479 results
-
Content Article
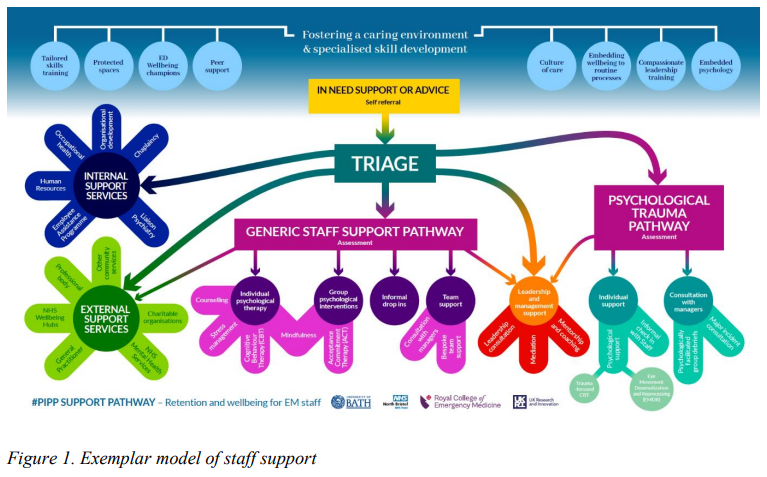 The Psychologically informed policy and practice development (PIPP) project investigated current workplace concerns, barriers to change and opportunities for development and growth, and was a collaborative project run by the Royal College of Emergency Medicine, UK Research and Innovation and the University of Bath. This document details specific evidence-based recommendations relating to four key areas identified as prioritised targets in emergency care workforce development: An environment to thrive in Cultivating a better culture A tailored pathway of care Enhanced leadership The recommendations are detailed, supported by evidence, existing guidelines and new empirical data, and are specific to the needs of the emergency care specialty.
The Psychologically informed policy and practice development (PIPP) project investigated current workplace concerns, barriers to change and opportunities for development and growth, and was a collaborative project run by the Royal College of Emergency Medicine, UK Research and Innovation and the University of Bath. This document details specific evidence-based recommendations relating to four key areas identified as prioritised targets in emergency care workforce development: An environment to thrive in Cultivating a better culture A tailored pathway of care Enhanced leadership The recommendations are detailed, supported by evidence, existing guidelines and new empirical data, and are specific to the needs of the emergency care specialty. -
Content ArticleFatigue refers to the issues that arise from excessive working time or poorly designed shift patterns. It is generally considered to be a decline in mental and/or physical performance that results from prolonged exertion, sleep loss and/or disruption of the internal clock. Fatigue results in slower reactions, reduced ability to process information, memory lapses, absent-mindedness, decreased awareness, lack of attention and underestimation of risk. It can lead to errors and accidents, ill-health and injury, and reduced productivity and is often a root cause of major accidents. This guidance from the Health and Safety Executive (HSE) outlines key information about fatigue and signposts to further resources about managing fatigue at work.
-
Content ArticleThe Health and Social Care Select Committee have published a new report reviewing the progress that the UK Government has made in implementing the recommendations of the Independent Medicines and Medical Devices Safety Review, sometimes referred to as the Cumberlege Review. This blog sets out Patient Safety Learning’s reflections on this report.
-
Content ArticleThis Health and Social Care Select Committee report reviews the progress that the UK Government has made in implementing the recommendations of the Independent Medicines and Medical Devices Safety Review, sometimes referred to as the Cumberlege Review. You can read Patient Safety Learning’s reflections on this report here.
-
Content ArticleIn this blog, Judy Walker, an After Action Review (AAR) expert, looks at how effective learning from disasters and incidents can restore hope and trust, offering long-term improvements to systems that have failed. She talks about how public inquiries, although they can seem frustratingly slow, benefit society when the relevant authorities ensure that learning is understood and implemented. She compares this to the impact of AARs, highlighting that people’s trust in the process is linked to their perception of the changes that happen as a result of the AAR. She outlines three steps that NHS providers should take to ensure the AAR process is effective in restoring hope: Highlight to all staff on a regular basis, the benefits that are being delivered due to AARs Ensure patients and family members are provided with specific information about how AARs prevent future harms Support the people who lead AARs to do so skilfully, so that quality is assured and staff can trust in the safety and value of the process.
-
Content ArticleIn the UK, the focus of osteoporosis care in the NHS has been on people who have sustained a fragility fracture as a result of their underlying condition. Not much has been done to try and prevent the first fracture by promoting good bone health and proactively identifying people at higher risk. This report by the APPG on Osteoporosis and Bone Health presents the results of its inquiry into primary care provision for people with osteoporosis and those at high risk of fracture, launched in March 2022. The inquiry aimed to establish the current quality of care being offered to patients.
-
Content ArticleRecording of the Health and Social Care Committee meeting held on Tuesday 13 December 2022. Meeting started at 10.03am, ended 11.45am.
-
Content ArticleThis policy paper, published by the Department of Health and Social Care, provides an update on the UK Government’s progress in implementing the recommendations of the Independent Medicines and Medical Devices Safety (IMMDS) Review, sometimes referred to as the Cumberlege Review.
- Posted
- 3 comments
-
- (and 6 more)
-
Content ArticleAn expert review of the clinical records of 44 deceased patients who had been under the care of neurologist Dr Michael Watt has found there were “significant failures” in their treatment and care. Dr Watt, a former Belfast Health and Social Care Trust consultant neurologist, was at the centre of Northern Ireland’s largest ever recall of patients, which began in 2018, after concerns were raised about his clinical work. More than 4,000 of his former patients attended recall appointments. At the direction of the Department of Health, in August 2021, the Regulation and Quality Improvement Authority (RQIA) commissioned the Royal College of Physicians to undertake an expert review of the clinical records of certain deceased patients who had been under the care of Dr Watt, with the intention to understand his clinical practice, to ensure learning for others and to help make care better and safer in the future.
-
Content ArticleKeeping patients safe during their care and treatment should be at the heart of any health system, including the NHS. Yet avoidable harm still occurs every day, around the world. There have been major efforts to prioritise patient safety in England, but the pandemic has shone a light on areas of care where progress has stalled, or safety has deteriorated. This report by Imperial College London's Institute of Global Health Innovation, commissioned by Patient Safety Watch, brings together publicly available data to present a national picture of patient safety in England.
- Posted
- 1 comment
-
- (and 9 more)
-
News Article
Concern voiced over 'unacceptably high level' of births by caesarean section

Patient Safety Learning posted a news article in News
The rising number of women who have caesarean sections instead of natural births is causing concern for the National Childbirth Trust (NCT). The trust, which supports women through pregnancy, childbirth and early parenthood, says it does not know why the rate of caesareans is increasing. One in four maternity services showed a caesarean rate of between 20% and 29.9%, and 2% of services had a rate of more than 30%, according to latest figures. The World Health Organization recommends that the acceptable rate is 10 to 15%. The maternity care working party, a multi-disciplinary group set up by the NCT, said there was an urgent need to address the problem. "A caesarean is major abdominal surgery," the working party said in a statement to a conference in London with the Royal College of Midwives and the Royal College of Obstetricians and Gynaecologists "Most women would prefer to give birth normally, provided that a normal birth is considered safe for them and their baby. It is important that health professionals' advice does not have the effect of denying them this opportunity without good reason." The working party is calling for data to be published on caesarean section rates and for obstetricians to justify in each case that the benefits outweigh the hazards. It also wants action to be taken to prevent any inappropriate use of caesarean sections. Belinda Phipps, chief executive of the NCT, said: "We know that in many cases caesareans are necessary for good clinical reasons. However, in our view rates have reached unacceptable levels and we want to know why." Read full story Source: The Guardian, 24 November 2022- Posted
- 1 comment
-
- (and 3 more)
-
Content ArticleThis cross-sectional study in BMJ Evidence-Based Medicine aimed to understand the relationship between financial conflicts of interest and recommendations for atrial fibrillation (AF) screening in the UK. The authors looked at whether the UK media recommend for or against screening for AF and the financial conflicts of interests of AF screening commentators. The authors found that the vast majority of UK media promotes screening for AF, in contrast to the position of the independent UK National Screening Committee, which recommends against screening. Most commentators, internal NHS organisations and UK charities promoting screening had a direct or indirect financial conflict of interest. Independent information was rare and the reasons for this are unknown. They recommend readers consider the potential impact of financial conflicts on recommendations to screen.
-
Content ArticleOn 1 November 2022, Dr Bill Kirkup, HSIB's Clinical Director of Maternity Investigations, and lead investigator for the investigation into maternity and neonatal services at East Kent Hospitals University NHS Foundation Trust, presented the investigation report: 'Reading the signals' in a seminar delivered to HSIB staff.
-
Content Article
 Published on 19 October 2022, the report of the investigation into maternity and neonatal services at East Kent Hospitals NHS Foundation Trust revealed a series of serious patient safety failings between 2009 and 2020, which resulted in avoidable harm to patients and deaths. The investigation found that if nationally recognised standards had been followed, the outcome could have been different in 97 of the 202 cases reviewed. In this article, Patient Safety Learning analyses the findings of this report from a broad patient safety perspective, focusing on five key themes that are consistent with many other serious patient safety inquiries and reports in recent years. It sets these in their wider context and highlights the need for a fundamental transformation in our approach to patient safety if similar scandals are to be prevented in the future.
Published on 19 October 2022, the report of the investigation into maternity and neonatal services at East Kent Hospitals NHS Foundation Trust revealed a series of serious patient safety failings between 2009 and 2020, which resulted in avoidable harm to patients and deaths. The investigation found that if nationally recognised standards had been followed, the outcome could have been different in 97 of the 202 cases reviewed. In this article, Patient Safety Learning analyses the findings of this report from a broad patient safety perspective, focusing on five key themes that are consistent with many other serious patient safety inquiries and reports in recent years. It sets these in their wider context and highlights the need for a fundamental transformation in our approach to patient safety if similar scandals are to be prevented in the future.- Posted
- 3 comments
-
2
-
- (and 11 more)
-
Content ArticleThe APPG held their annual general meeting in Parliament. Baroness Cumberlege was re-elected as Co-Chair of the group and in light of Jeremy Hunt’s recent appointment as Chancellor of the Exchequer, Sharon Hodgson MP was elected as Co-Chair, having previously supported the Group as Vice-Chair over the last calendar year. Sharon is is an Officer of the APPG for Valproate and other Anti-Epileptic Drugs in Pregnancy and Vice-Chair of the All-Party Parliamentary Group on Surgical Mesh. The current serving Vice-Chairs were re-elected, with the addition of Baroness Ritchie also joining as Vice-Chair. The Group looked back on a year of significant activity and progress, including the appointment of Dr Henrietta Hughes as the first Patient Safety Commissioner in England, and agreed that a renewed focus on seeking the implementation of redress schemes should be a priority for the Group over the next year.
-
Content Article
How can Parliament make health and care safer for all? (4 November 2022)

Mark Hughes posted an article in Others
In this blog for the cross-party think tank Policy Connect, the Professional Standards Authority for Health and Social Care sets out its view on the biggest challenges affecting the quality and safety of health and social care outlined in its report Safer care for all - solutions from professional regulation and beyond. It describes gaps in the wider framework to protect the public highlighted in this report and considers where Parliament and the Government have an opportunity to act to support safer care for all. Related reading Patient Safety Learning: Joining up a fragmented landscape: Reflections on the PSA report ‘Safer care for all’ (12 September 2022) Working together to achieve safer care for all: a blog by Alan Clamp (12 September 2022) -
Content ArticleBipolar UK's 'Bipolar Minds Matter' report calls for an immediate restructure of the healthcare system that is failing millions affected by bipolar, and puts forward the case for developing a dedicated care pathway so that people with bipolar can have access to specialist treatment and continuity of support over a lifetime.
-
Content ArticleIn 2021-22 the House of Commons Health and Social Care Select Committee held an inquiry into Cancer services, asking for evidence of why cancer outcomes in England continue to lag behind comparable countries internationally and examine evidence relating to the underlying causes of these differences. This document was submitted by Pancreatic Cancer UK as part of the call for written evidence in this inquiry.
-
Content ArticleIf you want to find out what the new Patient Safety Incident Response Framework is all about, and how it will support the NHS to learn and improve, this video provides a helpful introduction.
-
Content Article
 In this short blog, Patient Safety Learning sets out its initial response to the publication of the report of the independent investigation into maternity and neonatal services at the East Kent Hospitals NHS Foundation Trust.
In this short blog, Patient Safety Learning sets out its initial response to the publication of the report of the independent investigation into maternity and neonatal services at the East Kent Hospitals NHS Foundation Trust.- Posted
- 1 comment
-
1
-
- (and 7 more)
-
Content ArticleIn February 2020 the UK Government commissioned Dr Bill Kirkup to undertake a review into maternity and neonatal care services between 2009 and 2020 in two hospitals, the Queen Elizabeth The Queen Mother Hospital (QEQM) at Margate and the William Harvey Hospital (WHH) in Ashford. Both these services fall under the East Kent Hospitals NHS Foundation Trust. The report found that over this period those responsible for these services too often provided clinical care that was suboptimal and led to significant harm, failed to listen to the families involved, and acted in ways which made the experience of families unacceptably and distressingly poor. It identifies four key areas for action which must be addressed to improve patient safety in maternity and neonatal care services.
-
News ArticleA key national policy change recommended by the inquest which led to the East Kent maternity inquiry will not be implemented until next February – more than three years after it was called for by a coroner. The recommendation – that obstetric locum doctors be required to demonstrate more experience before working – was made in a prevention of future deaths report following the inquest into the death of seven-day-old Harry Richford at East Kent Hospitals University Foundation Trust. The remaining 18 recommendations from the PFD report were requiring specific actions by the trust, rather than national policy makers. The trust says they have been implemented. However, NHS England and the Royal College of Obstetricians and Gynaecologists have only in recent months produced guidance on using short-term locums in these services, and it will not come into effect until February. When it does, it will require them to complete a certification of eligibility, demonstrating they have had recent experience in a number of clinical situations, including complex Caesarean sections. Middle-grade locums have until next February to gain the certificate. The independent inquiry into maternity at the trust – prompted by Harry’s death – will report tomorrrow, Wednesday 19 October, and is expected to be highly critical of the trust, and of national efforts to make services safe over recent years. Read full story (paywalled) Source: 18 October 2022
-
News Article
East Kent NHS inquiry finds better care might have prevented 45 babies’ deaths
Patient Safety Learning posted a news article in News
The deaths of at least 45 babies could have been avoided if nationally recognised standards of care had been provided at one of England’s largest NHS trusts, a damning inquiry has found. Dr Bill Kirkup, the chair of the independent inquiry into maternity at East Kent hospitals university NHS foundation trust, said his panel had heard “harrowing” accounts from families of receiving “suboptimal” care, with mothers ignored by staff and shut out from discussions about their own care. The inquiry’s report said: “An overriding theme, raised with us time and time again, is the failure of the trust’s staff to take notice of women when they raised concerns, when they questioned their care, and when they challenged the decisions that were made about their care.” Of 202 cases reviewed by the experts, the outcome could have been different in 97 cases, the inquiry found. In 69 of these 97 cases, it is predicted the outcome should reasonably have been different and it could have been different in a further 28 cases. Of the 65 babies’ deaths examined, 45 could have had a different outcome if nationally recognised standards of care had been provided. In nearly half of all cases examined by the panel, good care could have led to a different outcome for the families. Some of the bereaved parents accused the trust of “victim blaming” mothers for their children’s deaths. Kelli Rudolph and Dunstan Lowe, whose daughter Celandine died at five days old, said: “Doctors sought to blame Kelli for Celandine’s death. This victim blaming was the first in a long line of interactions with those in the trust who sought to delay, deflect and deny our search for the truth about what happened to our baby. “In isolation, these tactics traumatised us after the tragedy of our daughter’s death. But when seen in the light of 10 years of failures, they signal a concerted effort to cover up the trust’s responsibility for what happened to Celandine and the many others who lost their lives due to failures in clinical judgment.” Read full story Source: The Guardian. 19 October 2022 -
News ArticleIn 2018 the British Association of Aesthetic Plastic Surgeons (www.baaps.org.uk) dissuaded all its members from performing Brazilian Buttock Lift (BBL) surgery, until more data could be collated. The decision was taken due to the high death rate associated with the procedure. Now, following an extensive four-year review of clinical data, new technology and techniques, BAAPS has published its Gluteal Fat Grafting (GFG) guidelines. Gluteal fat grafting is currently the procedure with the biggest growth rate in plastic surgery worldwide, with an increase of around 20% year-on-year). It has become the most popular means of buttock volume augmentation, overtaking gluteal augmentation with implants. In 2020, The Aesthetic Society statistics recorded 40,320 buttock augmentation procedures, which included both fat grafting and buttock implants. In 2015, there were reports of intraoperative mortality related to pulmonary fat emboli associated with BBL surgery and in 2018 with growing concern about the high mortality rate associated with this procedure BAAPS recommended it was not performed by its members. The development of the present guidelines and recommendations has been stimulated by the evidence that has emerged since 2018, based on scientific review and analysis. BAAPS guidelines now recommend that Gluteal Fat Grafting is safe to perform under two key conditions: Injection into the subcutaneous plane only - there is a plethora of evidence to suggest this significantly reduces mortality related to the procedure perhaps this needs to be changed to – the evidence shows that the only deaths from the procedure have been when fat has been injected into the deeper muscle layer. Intraoperative ultrasound must be used during the placement of fat in the gluteal area to ensure that the cannula remains in the subcutaneous plane – this is the only way that surgeons can be confident they are not in the muscle layer. Read full story Source: BAAPS, 17 October 2022
-
Content ArticleA thematic review can identify patterns in data to help answer questions, show links or identify issues. Thematic reviews typically use qualitative (e.g, open text survey responses, field sketches, incident reports and information sourced through conversations and interviews) rather than quantitative data to identify safety themes and issues. Thematic reviews can sometimes use a combination of qualitative data with quantitative data. Quantitative data may come from closed survey responses or audit, for example. These top tips support health and social care staff to carry out thematic reviews, but organisations may take different approaches, depending on the purpose and scope of their review.






