
Summary
Chris Elston, a patient safety education lead, shares how he used Safety Engineering Initiative for Patient Safety (SEIPS) and Accident Mapping (AcciMap) to learn from a patient safety incident at his Trust.
Content
The incident
At a recent Patient Safety Education Network meeting, I shared this slide. It was the first meeting of the year and this seemed to meet one of our objectives – to share learning from incidents. In truth, I expected the discussion to last no longer than 10 minutes and there would be minimal involvement. I was shocked that when I checked my watch 40 minutes had passed.

This incident has been through a case review meeting, colloquially known as a scoping meeting. This consists of a medical lead for scoping, patient safety team representation, divisional governance representation and members of the team that were involved in the incident. It could be viewed as a mini multidisciplinary team review.
During the discussion there was the usual sort of questions: Was it a Patient Safety Incident Investigation (PSII) or a local learning response (LLR)? What tools were used? How was the learning shared? But there was one question that made me stop and think. How can we use this incident to improve the use and understanding of some of the new tools within the Patient Safety Incident Response Framework (PSIRF)? So here goes, hopefully a short piece to help with the application of two tools – Safety Engineering Initiative for Patient Safety (SEIPS) and Accident Mapping (AcciMap).
AcciMap
AcciMap or Accident Mapping is a tool developed by Rasmussen in 1997.[1] It was originally produced to be used in the transport arena and has different levels: (1) Government, legislation and budgeting; (2) Regulatory bodies and Associations; (3) Local Government, company management, planning and budgeting; (4) Technical and operational management; (5) Physical processes and actor activities; and (6) Equipment and surroundings. We have modified it a little and have only five levels.
- External factors – NHSE directives, targets, government targets, media influences, Integrated Care Board priorities, pandemics, social circumstances, public awareness and expectations.
- Organisational factors/hospital management – included here would be culture, policies, guidelines, change management strategies, pressures to perform, multi-site working and culture.
- Technical and operational management (job/workplace factors) – included here will be the individual workplace items such as lack of equipment, tools and technology being used, environment, staffing levels and rotas.
- Physical/individual factors – these can be for any of the 'players' in the incident and would include experience, training, skills, tiredness, hunger, emotions, to name a few.
- Outcome – poor or good and can be multiple outcomes.
It should be noted that these are not exhaustive lists but more a flavour of what can be covered in each level. I do take the view that there are no wrong 'answers' with an AcciMap and it is more important to get the contributory factors down on the chart, to then be able to examine the interactions. So, what did this look like for the patient safety incident? Something like this:

You can now see potential interactions. Let's pick one element of the AcciMap; for example, if we look at how the Nursing and Midwifery Council (NMC) Preceptorship Standards may influence what happened in this incident. The NMC standards may be incorporated into the hospital policy and this in turn may dictate the ideal staffing levels. With these levels sorted out, then adequate support and supervision can be provided to junior staff members. So, there may be some work to see these interactions.
There is an additional negative interaction on the staffing levels, which is from the media focus on maternity units and healthcare in general. These negative headlines could be influencing the recruitment of students to midwifery and nursing programmes, but also the staffing levels may be influencing on where students are applying for jobs when they graduate. There will be many other interactions that require further investigation with other tools, such as observations, Walk Through, Talk Through, and possibly exploration in interviews.
There is a positive outcome throughout all of this, and that is the teamwork and the co-ordination of three specialist teams in the care of the child – ortho, plastics and general surgery. They all came together to offer their expert opinion so, even though we start with a negative outcome, there is a glimmer of hope in the incident. This is shown with the green arrows and box.
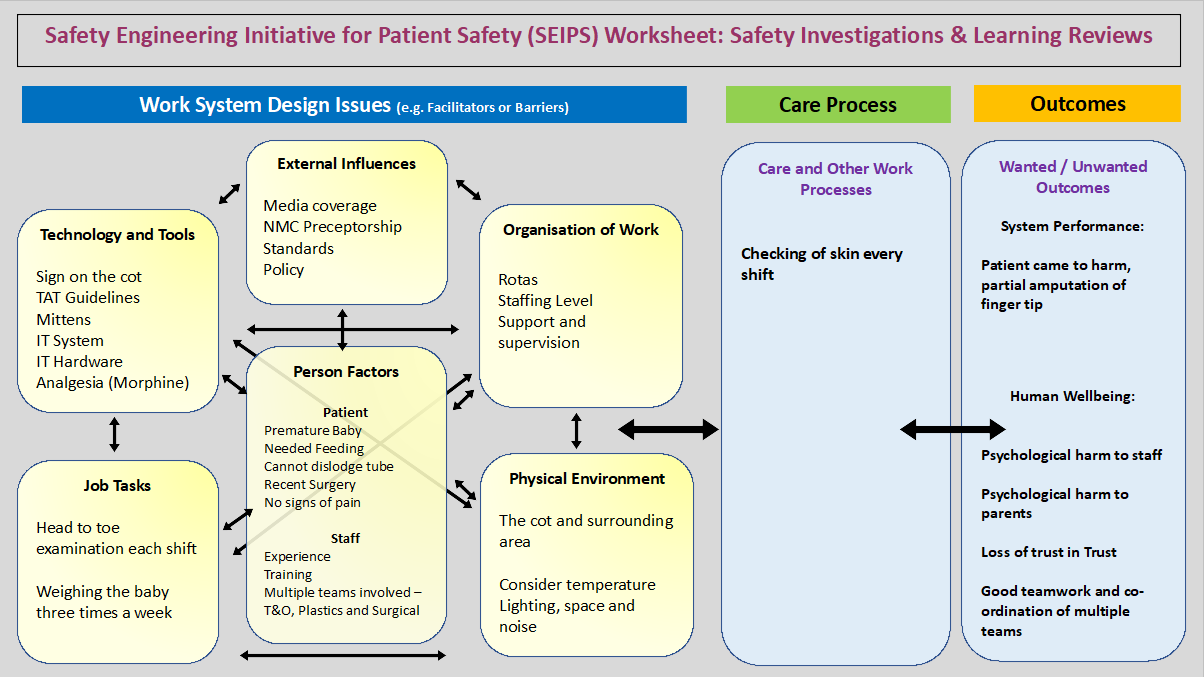
Systems Engineering Initiative for Patient Safety (SEIPS)
We can now turn our attention to the SEIPS framework. We need to remember that this is another framework and not an investigative tool in itself. What I mean is that this is a way to highlight potential interactions and how they may affect the processes and outcomes.

So if we follow a thread on the SEIPS, we can see that the outcome was influenced by the care process of checking the skin every shift, but in this case there is no record of this. So we may discuss this with the practitioner and ask their level of experience, how they interact with the IT system and if there are enough computers, laptop and desktop or IPADs to record this at the time that it is done. What was there understanding of the sign that states 'Babies are to be nursed with mittens on at all times'? Does this allow for the mittens to be removed to check the skin? What do other members of staff do and understand by this?
I think that both frameworks highlight potential interactions, then you hang other tools on the frame to get into the world of work as done. I imagine as we in healthcare get more used to the tools, that they will evolve and mature.
Actions and next steps
Following this incident, the following changes have been made:
- All donated mittens are now checked for loose threads.
- We are looking at whether the use of babygrows with integral mittens would be a more feasible option. Advising parents that this is the best option for their children may reduce the cost pressure on the Trust, whilst ensuring the child gets the requisite protection following the surgery. It would also mean that the parents would get long-term use from the clothing.
- The sign on the cot stating the 'must be nursed with mittens on at all times' has been changed to reflect the need for the mittens to be removed to facilitate the skin check, once a shift.
- The information has been shared at the local Medical Devices Safety Officer's forum to inform other local trusts of the risk and the patient safety incident we discovered.
- The neonatal team have also shared the event and the learning with the local maternity and neonatal network.
We provided a teaching session to the Patient Safety Management Network, where an AcciMap was written showing how the AcciMap can be used but also highlighting some good practice within the incident, namely the teamwork between three surgical specialities to ensure that the child got the best care possible after the event.
We also turned the multidisciplinary review into a SEIPS approach and provided a small amount of coverage about this. The pleasing aspect of this was the amount of discussion that it sparked. There were some questions and observations that had not been thought about. The discussion showed the value of a team approach with people that are not used to working on the team, who are able to notice the so-called basics that many of us take for granted.
One suggestion that came out from this would be to turn the process of a head to toe check into a hierarchical task analysis, so that may be something we do in the future.
Reference
Further information
- Carayon P, Schoofs Hunt A, Karsh B-T, et al. Work system design for patient safety: the SEIPS model. BMJ Quality Safety, 2006; 15: 50-58.
- Holden R, Carayon P, Gurses A, et al. SEIPS 2.0: A human factors framework for studying and improving the work of healthcare professionals and patients. Ergonomics, 2013; 56(11): 1669-1686.
- Carayon P, Wooldridge A, Hoonaker P, et al. SEIPS 3.0: Human-Centered Design of the Patient Journey for Patient Safety. Applied Ergonomics, 2020; 84.
- Holden R, Carayon P. SEIPS 101 and seven simple SEIPS tools. BMJ Quality and Safety, 2021; 30: 901-910.
- Waterson P, Jenkins D, Salmon P, Underwood P. ‘Remixing Rasmussen’: The evolution of Accimaps within systemic accident analysis. Applied Ergonomics, 2017; 59 Part B: 483-503.
Related reading on the hub
- Proxies for work-as-done: a blog series by Steven Shorrock, Humanistic Systems
- All Systems Ergo: Exploring SEIPS with Pascale Carayon
We would love to share more examples of how hub members are using the PSIRF tools to learn from a patient safety incident. Share your examples here (you will need to be a member of the hub, sign up is free and easy) or email us: [email protected].
About the Author
Chris Elston is Patient Safety Education Lead for University Hospital Southampton NHS Foundation Trust and Chair of the Patient Safety Education Network.
The Network is open to those who teach any element of patient safety or provide learning from patient safety incidents. The network is hosted on the hub. You can join by signing up to the hub today. When putting in your details, please tick ‘Patient Safety Education Network’ in the ‘Join a private group’ section. If you are already a member of the hub, please email [email protected].
1 Comment
Recommended Comments
Create an account or sign in to comment
You need to be a member in order to leave a comment
Create an account
Sign up for a new account in our community. It's easy!
Register a new accountSign in
Already have an account? Sign in here.
Sign In Now