Search the hub
Showing results for tags 'Patient safety incident'.
Found 682 results
-
News Article
GPs and patients invited to share views on legal ‘duty of candour’

Patient Safety Learning posted a news article in News
The Government is inviting views on how well GP practices and other NHS organisations are complying with their legal duty of candour when things go wrong. Patients and health professionals are being asked whether the statutory duty is well understood and adequately regulated by the CQC. Under the statutory duty of candour, introduced for all CQC-registered providers in 2015, GP practices must be open and honest with their patients when something goes wrong and has caused harm. In December, the Department of Health and Social Care (DHSC) announced a review into whether healthcare providers are following the duty of candour rules. This was in response to concerns that the duty is not always being met and that there is variation in how the rules are being applied. The DHSC has published its ‘call for evidence’ to gather views on how well the duty of candour obligation is working for both patients and health professionals. Patients have been asked whether GP practices and other providers ‘demonstrate meaningful and compassionate engagement’ with patients who have been affected by an incident. The call for evidence also asks for views on whether the criteria for triggering the duty are appropriate and well understood by staff. Read full story Source: Pulse, 16 April 2024 -
Content ArticleIncident reports of medication errors are valuable learning resources for improving patient safety. However, key information is often contained within unstructured free text, which prevents automated analysis and limits the usefulness of these data. Natural language processing can be used to structure this free text automatically and retrieve relevant past incidents and learning materials, but this requires a large, fully annotated and validated set of incident reports. This study in Nature used a set of 58,658 machine-annotated incident reports of medication errors to test a natural language processing model. The authors provide access to the validation datasets and machine annotator for labelling future incident reports of medication errors.
-
Content ArticleThose who use any type of health or social care service have a right to be informed about all elements of their care and treatment. Health and social care providers have that fundamental responsibility to be open and honest with those who are under their management and care. In particular, when things go wrong during the provision of care and treatment, patients and service users and their families or caregivers expect to be informed honestly about what happened, what can be done to deal with any harm caused, and to know what will be done to prevent a recurrence to someone else. In November 2014, the government introduced a statutory (organisational) duty of candour for NHS trusts and NHS foundation trusts via Regulation 20 of the Health and Social Care Act 2008. In essence, the duty places a direct obligation upon trusts to be open and honest with patients and service users, and their families, when something goes wrong that appears to have caused or could lead to moderate harm or worse in the future (known as a ‘notifiable safety incident’). The Department of Health and Social Care (DHSC) are seeking views on the statutory duty of candour for health and social care providers in England. This call for evidence closes at 11:59 pm on 29 May 2024.
-
Content ArticleWe know from several reports, reviews, and inquiries over recent years that the patient and family voice has not been heard. These voices are essential to learning and improvement because of their unique insight into how care is delivered. To improve safety we must understand its reality as experienced by patients. In a blog for the Patient Safety Commissioner website, Rosie Benneyworth, interim chief executive officer of the Health Services Safety Investigations Body (HSSIB), explains how HSSIB involves families in its investigations.
-
Content ArticleJudy Walker describes how an After Action Review following a sporting event ensured significant learning took place and led to a worldwide change in first aid training.
-
Content ArticleClinical guidelines can contribute to medication errors but there is no overall understanding of how and where these occur. This study aimed to identify guideline-related medication errors reported via a national incident reporting system, and describe types of error, stages of medication use, guidelines, drugs, specialties and clinical locations most commonly associated with such errors.
-
Content ArticleAs Rob Behren steps down as the Parliamentary and Health Service Ombudsman (PHSO) he records an episode of Radio Ombudsman, reflecting on his seven years in office. He also tells us about his early life, his career before PHSO and shares his future plans.
-
EventOur Human Factors – Applying to Incident Investigation programme is designed to equip staff with the knowledge and skills to use a systems approach to incident investigation. This is a great opportunity for programme participants to develop their understanding of Human Factors and apply this methodology to case studies with peers. The programme introduces the concept of system thinking and provides participants with the opportunity to discuss their own work context. Participants will grow their investigative mindset, whilst developing their knowledge and skills of the investigative process from the event timeline to recommendations for improvement. The programme also includes the opportunity to discuss and reflect on the essential components of good investigation, including; Being open and honest. Duty of candour. Co-designing investigations. Just culture. Systems based frameworks. Closing the loop from recommendations to action. Human Factors – Applying to Incident Investigation will take place on 9, 16 and 23 May 2024. Who is this for? The programme is aimed at all staff who are required to carry out or oversee incident investigation. Programme duration This is a 3 day programme. Delivery methods This programme is delivered virtually.
-
Content ArticleCentral to the Patient Safety Incident Response Framework (PSIRF) is the requirement for healthcare organisations to be proactive in how they respond to and learn from patient safety incidents. This article from legal firm Kennedys considers the implications of PSIRF on healthcare organisations’ legal and governance teams. In particular, considering practical steps that may be adopted, as an example, in the context of preparing for an inquest.
-
Content ArticleThis leaflet produced by East London NHS Foundation Trust (ELFT) explains the Patient Safety Incident Response Framework (PSIRF) to patients and families, outlining the aims of PSIRF and what they can expect from the process.
-
Content Article
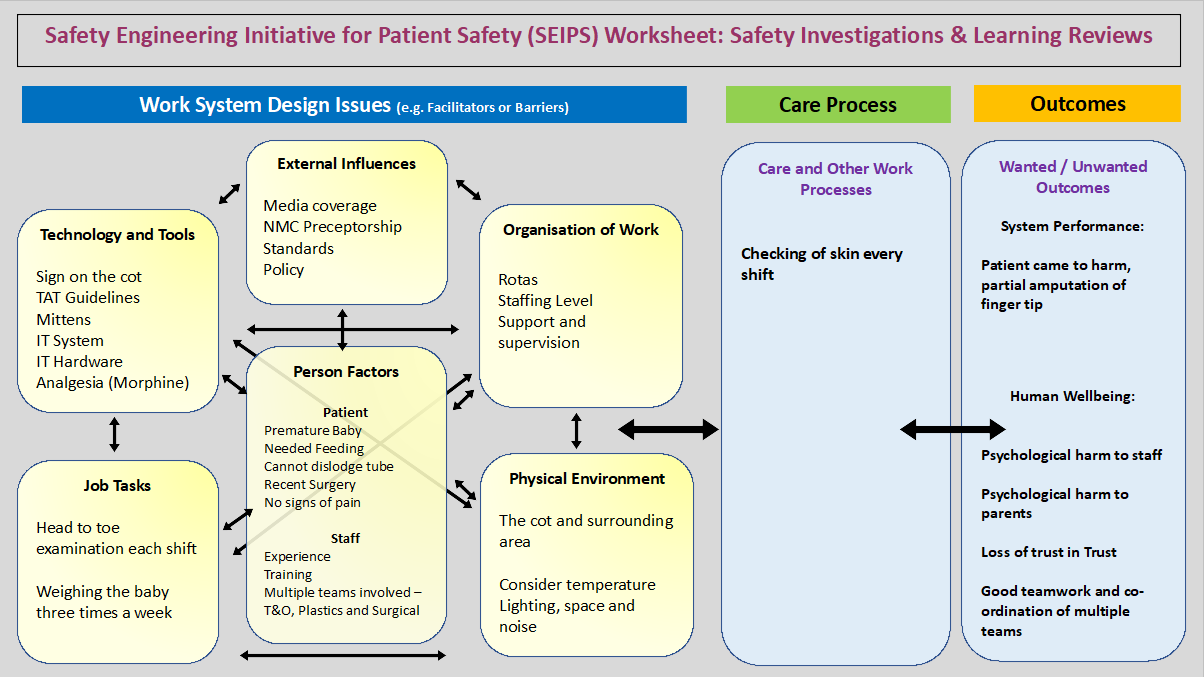 Chris Elston, a patient safety education lead, shares how he used Safety Engineering Initiative for Patient Safety (SEIPS) and Accident Mapping (AcciMap) to learn from a patient safety incident at his Trust.
Chris Elston, a patient safety education lead, shares how he used Safety Engineering Initiative for Patient Safety (SEIPS) and Accident Mapping (AcciMap) to learn from a patient safety incident at his Trust. -
Content ArticleFear of retaliation by leaders or colleagues can prevent staff from reporting adverse events, unsafe conditions, or near misses. This article presents strategies to improve just culture in the perioperative environment, which is prone to hierarchical structure. Strategies include creating an accessible reporting system, implementation of a "good catch" programme, and leadership support for staff who submit reports.
-
Event
The Patient Safety Incident Response Framework & clinical audit

Sam posted an event in Community Calendar
The Patient Safety Incident Response Framework (PSIRF) arguably represents the most significant change to investigating and managing patient safety incidents in the history of the NHS. To embed PSIRF effectively within organisations, healthcare teams need to understand and utilise a range of new techniques and disciplines. Clinical audit is an established quality improvement methodology that is often overlooked by patient safety teams, but will play an increasingly important role in ensuring that PSIRF fully delivers its stated objectives. CQC reports often highlight the importance of clinical audit as a measurement and assurance tool that can raise red flags if used appropriately. Indeed, both the Ockenden and Kirkup reports highlighted the importance of clinical audit in identifying and quantifying substandard care. While SEIPS, After Action Reviews, more in-depth interviewing techniques, etc. are all receiving much fanfare in relation to PSIRF, the importance of clinical audit needs to be better understood. This short course will explain how organisations who use clinical audit effectively will increase patient safety and better understand why incidents take place. We will look at the key role of audit in understanding work as imagined and works as done and show why national audits can assist with creating patient safety plans. Change analysis and the effective implementation of safety actions are keys to PSIRF delivery and clinical audit will assist in the delivery of both. We will also demonstrate the important, but often under-appreciated role, clinical audit staff will have in the successful delivery of PSIRF. Key learning outcomes: Why clinical audit is an integral element of PSIRF. Why clinical audit staff have a vital role to play in PSIRF. How clinical audit data can help raise red flags and spot risks. Using clinical audit to better understand your incidents. Ensuring your safety actions are working. Using audit to assess your patient safety incident investigations. Register -
Content ArticleThe Patient and Client Council’s role with respect to health and social care services is to: represent the interests of the public promote the involvement of the public; assist people making or intending to make a complaint through advocacy; promote the advice and information by HSC bodies to the public about the design, commissioning and delivery of services; undertake research into the best methods and practices for consulting and engaging the public.
-
Content ArticleThe Northern Ireland Public Services Ombudsman investigates unresolved complaints about public bodies in Northern Ireland. Before you make a complaint to us you should normally have: Complained directly to the organisation Gone through its complaints process Received a final response to your complaint. Their website will give you more information on what Northern Ireland Public Services Ombudsman do, how to make a complaint, and their investigations.
-
Content ArticleThe Regulation and Quality Improvement Authority (RQIA) are an independent health and social care regulator in Northern Ireland. RQIA aim to assure public confidence in health and social care through their independent, proportionate and responsible regulation. Through inspections, reviews and audits, RQIA provides assurance about the quality of care, challenges poor practice, promotes improvement and safeguards the rights of service users. RQIA informs the public of their findings through the publication of reports. They are committed to working closely with service providers so that they can deliver improved care and are dedicated to hearing and acting on the experiences of patients, clients, families and carers. This leaflet provides more information about RQIA.
-
Event
Systems approach to learning from patient safety incidents
Sam posted an event in Community Calendar
untilTraining to support the development of core understanding and application of systems-based patient safety incident response throughout the healthcare system - in line with NHS guidance, based upon national and internationally recognised good practice. This course covers the end-to-end systems-based patient safety incident response based upon the new NHS PSIRF and includes: purpose of patient safety incident response framework introduction to complex systems, system thinking and human factors restorative just and learning culture duty of candour involving staff in incident response involving patients, families and carers in incident response improvement science and developing system improvement plans general response techniques interviewing and asking questions conducting observations, understanding work as done systems frameworks response types patient safety investigation planning, analysis and report writing commissioning and oversight of an internal investigation a high-level overview of system-based response tools. Register -
Event
Systems approach to learning from patient safety incidents
Sam posted an event in Community Calendar
untilTraining to support the development of core understanding and application of systems-based patient safety incident response throughout the healthcare system - in line with NHS guidance, based upon national and internationally recognised good practice. This course covers the end-to-end systems-based patient safety incident response based upon the new NHS PSIRF and includes: purpose of patient safety incident response framework introduction to complex systems, system thinking and human factors restorative just and learning culture duty of candour involving staff in incident response involving patients, families and carers in incident response improvement science and developing system improvement plans general response techniques interviewing and asking questions conducting observations, understanding work as done systems frameworks response types patient safety investigation planning, analysis and report writing commissioning and oversight of an internal investigation a high-level overview of system-based response tools. Register -
Event
Systems approach to learning from patient safety incidents
Sam posted an event in Community Calendar
Training to support the development of core understanding and application of systems-based patient safety incident response throughout the healthcare system - in line with NHS guidance, based upon national and internationally recognised good practice. This course covers the end-to-end systems-based patient safety incident response based upon the new NHS PSIRF and includes: purpose of patient safety incident response framework introduction to complex systems, system thinking and human factors restorative just and learning culture duty of candour involving staff in incident response involving patients, families and carers in incident response improvement science and developing system improvement plans general response techniques interviewing and asking questions conducting observations, understanding work as done systems frameworks response types patient safety investigation planning, analysis and report writing commissioning and oversight of an internal investigation a high-level overview of system-based response tools. Register -
Content ArticleThe NHS regularly uses temporary staff to fill gaps in its workforce. This investigation explored the challenges of involving temporary clinical staff (bank only staff, agency staff and locum doctors working within trusts) in local trusts’ patient safety investigations. Trust-level investigations are important because they are a way to identify learning to improve healthcare systems, with the aim of reducing the potential for harm to patients. Identifying learning requires staff to be engaged in an investigation; if temporary staff are not involved, learning may be lost, posing a risk to patient safety. HSSIB identified this risk following analysis of serious incident reports provided by acute and mental health NHS trusts. To explore the issue further, the investigation carried out site visits and engaged with NHS trusts, providers of bank staff, agencies that supply staff to NHS trusts, substantive (permanent) NHS staff, bank and agency staff, and a range of national stakeholders.
-
Content ArticleFran Ives speaks with Pascale Carayon, a Professor in Industrial and Systems Engineering at the University of Wisconsin Madison. Pascale talks about her vision for the SEIPS (System Engineering Initiative for Patient Safety) framework, which she has been working on for many years. During the conversation, Pascale gives some valuable advice to those who are new to using SEIPS such as focussing on the interactions between the elements of the model, such as the organisation, the task, and the tools. Future possible developments for the framework were considered such as making a connection between patient safety and well-being such as stress and burnout.
-
Content ArticleThis report examined whether the NHS has been successful in improving the patient safety culture, encouraging reporting and learning from patient safety incidents.
-
Content ArticleOne of the major challenges of patient safety incident reporting and learning systems lies in the difficulties of extracting practical information from the vast amount of data collected. Furthermore, many countries have not started collecting incident reports in patient safety at national level which makes it difficult to identify avoidable patient safety incidents and take action on them nationally. Minimal Information Model for Patient Safety (MIM PS) has been developed to provide a simple tool to start collecting data on patient safety incidents to assist in data analysis and extract the minimal, but necessary information to learn from incidents in order to avoid recurrence of same types of incidents in the future. Also, the MIM PS can be used as mapping source from any types of existing reporting systems of patient safety incidents which means no need to develop the new reporting systems based on MIM PS. This MIM user guide aims to explain each MIM category and how to implement MIM. It went through a validation process with EU and EFTA countries in 2014-2015. The MIM PS validation was supported by European Union in which EFTA countries also participated in the pilot testing.
-
News Article
'Catastrophic' consequences after oxygen error
Patient Safety Learning posted a news article in News
A patient in north Wales suffered "catastrophic" consequences when staff didn't connect their oxygen supply correctly. The Betsi Cadwaladr health board, which was caring for the patient at the time, is investigating and says it was one of a small number of recent similar incidents. But it refused to say whether the patient died, or to explain what the “catastrophic” consequences were. It says it is working to improve staff training to avoid similar incidents happening again. On Tuesday, Wales' health minister Eluned Morgan said the health board still had "a lot to do," before it could be taken out of special measures. A report to the committee said: “Further patient safety incidents have occurred in the health board related to the preparation and administration of oxygen using portable cylinders. “On review, the cylinder had not been prepared correctly, resulting in no flow of oxygen to the patient. “One incident had a catastrophic outcome and is under investigation.” Read full story Source: BBC News, 20 February 2024 -
Content ArticleAlthough several studies have tried to quantify the cost of ‘adverse events’ in healthcare, the true costs remain unknown. To understand the ‘true cost’ of serious incidents, Jane Carthey argues we need to consider:The cost of additional treatment for the affected patient.The opportunity costs that accrue from reporting and managing incidents, claims and complaintsBusiness costs that accrue when, for example, healthcare staff are suspended.Costs resulting from implementing the duty of candour process, andPenalties and sanctions imposedIn other industries, the HSE’s Incident Cost Calculator is used to quantify the true costs of incidents. Inspired by this tool, Jane developed the Healthcare Serious Incident Cost Calculator. Available via the link below.


