Search the hub
Showing results for tags 'System safety'.
Found 517 results
-
News Article
Nurse's conviction should be wake-up call for health system leaders, IHI says

Patient Safety Learning posted a news article in News
RaDonda Vaught's conviction for a fatal medical error has already damaged patient safety and should serve as a wake-up call for health system leaders to improve harm prevention efforts, the Institute for Healthcare Improvement has said. Ms. Vaught was convicted 25 March of criminally negligent homicide and abuse of an impaired adult for a fatal medication error she made in December 2017 while working as a nurse at Vanderbilt University Medical Center in Nashville, Tenn. "We know from decades of work in hospitals and other care settings that most medical errors result from flawed systems, not reckless practitioners," IHI said. "We also know that systems can learn from errors and improve, but only when those systems encourage reporting, transparently acknowledge their mistakes and are held accountable for those errors." The organization said criminal prosecution of errors over-focuses on the individual and diverts attention from necessary system-level issues and improvements. "Were this practice to be repeated in future cases of a serious or fatal error, there will be more damage, less transparency, less accountability and more lives lost," IHI said. "Instead, this case should be a wake-up call to health system leaders who need to proactively identify system faults and risks and prevent harm to patients and those who care for them." -
News Article
Gloucestershire CQC inspection highlights urgent care delays
Patient Safety Learning posted a news article in News
An inspection of a county's urgent and emergency services found delays were caused by a lack of empty beds and prolonged waiting times. The Care Quality Commission (CQC) inspected Gloucestershire emergency care services in November and December. The report found staff worked well in challenging circumstances but the CQC said pressures on workers across the system needed addressing. Dr Jeremy Welch said: "The system is being stretched and we need to adapt." CQC deputy chief inspector for hospitals, Nigel Acheson, said: "We found the system to be complicated. As a result, staff and patients weren't always able to understand which urgent and emergency care service was best suited to their needs. "This meant people sometimes attended the emergency department when they could have been treated more appropriately elsewhere." In addition the report touched on adult social care and the possibility of using empty care home beds when hospitals were struggling to cope. Dr Welch recognised "it's been a blinking tough time in care homes" over the pandemic and credited the relaxing of rules to allow visits but said there are other factors that would need to be considered. However he added: "We've got enough beds when we map across, it's just getting patients through the hospital and home because home is where they want to be." Read full story Source: BBC News, 17 March 2022 -
News Article
Tackle hidden racism in the NHS to improve staffing

Patient_Safety_Learning posted a news article in News
Racism is a significant issue affecting recruitment, retention, and patient care. With this in mind, the Royal College of Psychiatrists launched the Act Against Racism campaign, offering guidance and actions to combat racism in the workplace for better staff well-being and patient care, writes Adrian James In June, HSJ revealed that mental health trusts in England are among the biggest users of locum doctors in the NHS. With one in seven medical posts in mental health trusts vacant, many providers now rely on locum doctors to deliver essential services to patients. Read full story Source: HSJ, 9 August 2023 -
News ArticlePatients are at risk of a missed cancer diagnosis due to a reliance on paper records, an NHS trust has admitted after a man died due to his tumour being overlooked. Michael Lane, 50, from Shrewsbury, was “failed” by Shrewsbury and Telford Hospital Trust, his family has said after his cancer scan result was misplaced leaving him with a growing kidney tumour for 10 years. The trust is yet to fully launch an electronic record system a year after an investigation into Mr Lane’s death warned other patients were at risk due to the gap in paper records. Mr Lane went into Shrewsbury and Telford Hospital for a scan following a referral for suspected cancer in 2011. The radiographer flagged a small tumour but the scan was overlooked, placed within his paper records and never reported as being a concern. In an investigation report carried out by the trust in May 2021, seen by The Independent, the hospital admitted that had his tumour been seen and operated on earlier he may have survived. The report also admitted there were ongoing risks within the trust due to gaps in its electronic records system. It said: “The implementation of an IT solution will not prevent sad cases such as that of Mr Lane where the scan report that was missed took place before the widespread availability of such systems, however, it is clear that until we have an electronic requesting and sign-off system we remain at risk of new cases of missed results and harm occurring as a result of the ongoing reliance of paper-based results.” Read full story Source: The Independent, 17 July 2022
-
News Article
Medical expert witnesses ‘should not scapegoat doctors’
Patient Safety Learning posted a news article in News
Medical experts in cases involving doctors should have a mandatory duty to consider systems issues such as inadequate staffing levels to avoid them being scapegoated for wider failures, the Medical Protection Society (MPS) has said. The MPS, which supports the the professional interests of more than 300,000 healthcare professionals around the world, says medical expert reports focus on scrutinising the actions of the individual doctor even when failings are a result of the setting in which they work. Its report on the issue, shared with the Guardian before publication, points out that for doctors “adverse opinion can lead to loss of career or liberty”. It references the case of Dr Hadiza Bawa-Garba who was convicted of gross negligence manslaughter in 2015 and handed a 24-month suspended sentence for her part in the death of six-year-old Jack Adcock from sepsis. She was later struck off by the General Medical Council before the court of appeal overturned the GMC’s decision. Dr Rob Hendry, the MPS medical director, said: “In giving an opinion on whether or not the care provided by a doctor has fallen short of a reasonable standard, it would seem fair to the doctor that the medical expert considers all relevant circumstances. Any individual performance concerns must of course be addressed, but doctors should not be scapegoats for the failings of the settings in which they work. Sadly, we see this all too often in cases against doctors … “Many expert reports focus solely on the actions of the individual without considering the wider context. In reality, patient harm arising from medical error is rarely attributable to the actions of a single individual. Inadequate staffing levels, lack of resources, or faulty IT systems are just some issues which can contribute to adverse incidents. Doctors confront these issues every day and have little influence over them.” Read full story Source: The Guardian, 18 July 2022 -
News Article
Northern Ireland: Serious adverse incidents 'likely to be repeated'
Patient Safety Learning posted a news article in News
Health Minister Robin Swann has announced plans to improve the review process for serious adverse incidents (SAI) in Northern Ireland's health and social care system. The reviews take place after unintended incidents of harm and ensure improvements are made. The Regulation and Quality Improvement Authority (RQIA) was commissioned to examine the system's effectiveness. It found the process was not "sufficiently robust". In the RQIA report, the independent body found that "neither the SAI review process nor its implementation is sufficiently robust to consistently enable an understanding of what factors, both systems and people, have led to a patient or service user coming to harm". It added: "The reality is that similar situations, where events leading to harm have been inadequately investigated and examples of recognised good practice have not been followed, have been and are likely to be repeated in current practice." It identified failures in the SAI procedure, including failures to: Answer patient and family questions. Determine where safety breaches have occurred. Achieve a systemic understanding of those safety breaches. Design recommendations and action plans to reduce the opportunity for the same or similar safety breaches in future. Read full story Source: BBC News, 7 July 2022 -
News Article
Covid’s effect on mental health not as great as first thought, study suggests
Patient Safety Learning posted a news article in News
Covid-19 may not have taken as great a toll on the mental health of most people as earlier research has indicated, a new study suggests. The pandemic resulted in “minimal” changes in mental health symptoms among the general population, according to a review of 137 studies from around the world led by researchers at McGill University in Canada, and published in the British Medical Journal. Brett Thombs, a psychiatry professor at McGill University and senior author, said some of the public narrative around the mental health impacts of Covid-19 were based on “poor-quality studies and anecdotes”, which became “self-fulfilling prophecies”, adding that there was a need for more “rigorous science”. However, some experts disputed this, warning such readings could obscure the impact on individual groups such as children, women and people with low incomes or pre-existing mental health problems. They also said other robust studies had reached different conclusions. Read full story Source: The Guardian, 8 March 2023 -
News Article
NHS warned over writing to patients in English after child dies
Patient Safety Learning posted a news article in News
Patient safety investigators have issued a warning to the NHS over writing to patients only in English after a Romanian child died following missed cancer scans. The three-year-old, of Romanian ethnicity, had an MRI scan delayed after they were found to have eaten food beforehand. When the appointment for the child’s MRI scan was made by the radiology booking team, a standard letter was produced by the NHS booking system in English asking the child not to eat before the scan, despite the family’s first language being Romanian. Staff at the trust had hand-written on the patient’s MRI request sheet that an interpreter was required. “The family recognised key details in the written information, including the time, date and location of the scan,” the report said. “However, they were not able to understand the instructions about the child not eating or drinking (fasting) for a certain amount of time before the scan.” The Healthcare Safety Investigation Branch (HSIB) has urged NHS England to develop and implement new rules on supplying written appointment information in languages other than English. Read full story Source: The Independent, 27 April 2023 -
Content ArticleSystem working (which includes health and care) is the only way the NHS can address the interlinked problems of struggling primary care, elective backlog, ambulance and emergency department overload, and delayed discharge. In this HSJ article, Len Richards explains how system working grows from the right culture, clinical leadership and systemwide joined up, real-time data.
-
Content Article
 This is part of our series of Patient Safety Spotlight interviews, where we talk to people working for patient safety about their role and what motivates them. Rob talks to us about his passion for using human factors to improve safety in emergency departments, how allowing doctors to choose their own shifts can make staffing safer and how better integrating technology could help doctors diagnose and treat patients more safely and effectively.
This is part of our series of Patient Safety Spotlight interviews, where we talk to people working for patient safety about their role and what motivates them. Rob talks to us about his passion for using human factors to improve safety in emergency departments, how allowing doctors to choose their own shifts can make staffing safer and how better integrating technology could help doctors diagnose and treat patients more safely and effectively. -
Content ArticleQuality improvement is a methodology used routinely in emergency departments (EDs) to bring about change to improve outcomes such as waiting times, time to treatment and patient safety. However, introducing the changes needed to transform the system in this way is seldom straightforward with the risk of “not seeing the forest for the trees” when attempting to make changes. This article in Annals of Emergency Medicine aims to demonstrate how the functional resonance analysis method can be used to capture the experiences and perceptions of frontline staff to identify the key functions in the system (the trees), to understand the interactions and dependencies between them to make up the ED ecosystem (“the forest”) and to support quality improvement planning, identifying priorities and patient safety risks.
-
Content ArticleAgainst the backdrop of the Covid-19 pandemic, ensuring the safety of health and social care services remains a serious, ongoing challenge. This report examines how patient safety governance mechanisms in Organisation for Economic Co-Operation and Development (OECD) countries have withstood the test of Covid-19. It provides recommendations for further improving patient safety governance and strengthening health system resilience in OECD countries. This working paper was produced by the OECD for the 5th Global Ministerial Summit on Patient Safety, held in Montreux, Switzerland in February 2023.
-
Content ArticleAfter Steve Burrow’s mother was harmed by medical care in Wisconsin, he took time out from his successful film career to advocate for her. In this episode of Lit Health, he touches upon his fascinating career, why stories matter, and delves deeply into his experience with the medical system, its need for policy reform and the role he has taken on as an advocate in this space with host, Tracy Granzyk. Lit Health podcasts interview authors, healthcare leaders, and policymakers working to create a healthcare environment that is equitable, transparent, and that welcomes the needs of every patient – especially our vulnerable populations including the mentally ill, people of colour and women who feel they are at risk in our current system, the elderly, and anyone who feels bias or the isms affect their health and quality of life. You can also watch Steve Burrow's documentary: Bleed Out,
-
Content Article
 ‘Human factors’ is the science of improving performance by understanding individual or team behaviour and cognitive biases. This can allow a redesign of clinical systems and environments to improve patient safety. This course aims to help healthcare professionals understand human factors in complex healthcare setting and can be delivered as a full day, half day or a conference talk. It was developed by Professor Robert Galloway, Emergency Medicine Consultant at University Hospitals Sussex NHS Trust. The course covers: the principles of ‘human factors’–why errors occur. human cognitive biases (in memory, reasoning, decision-making). practical skills and tools to improve individual/team performance and patient safety. You can email Rob Galloway for more information on booking this course.
‘Human factors’ is the science of improving performance by understanding individual or team behaviour and cognitive biases. This can allow a redesign of clinical systems and environments to improve patient safety. This course aims to help healthcare professionals understand human factors in complex healthcare setting and can be delivered as a full day, half day or a conference talk. It was developed by Professor Robert Galloway, Emergency Medicine Consultant at University Hospitals Sussex NHS Trust. The course covers: the principles of ‘human factors’–why errors occur. human cognitive biases (in memory, reasoning, decision-making). practical skills and tools to improve individual/team performance and patient safety. You can email Rob Galloway for more information on booking this course. -
Content ArticleThis paper aims to highlight how to reduce medication errors through the implementation of human factors science to the design features of medication containers. Despite efforts to employ automation for increased safety and decreased workload, medication administration in hospital wards is still heavily dependent on human operators (pharmacists, nurses, physicians, etc.). Improving this multi-step process requires its being studied and designed as an interface in a complex socio-technical system. Human factors engineering, also known as ergonomics, involves designing socio-technical systems to improve overall system performance, and reduces the risk of system, and in particular, operator, failures. The incorporation of human factors principles into the design of the work environment and tools that are in use during medication administration could improve this process. During periods of high workload, the cognitive effort necessary to work through a very demanding process may overwhelm even expert operators. In such conditions, the entire system should facilitate the human operator’s high level of performance. Regarding medications, clinicians should be provided with as many perceptual cues as possible to facilitate medication identification. Neglecting the shape of the container as one of the features that differentiates between classes of medications is a lost opportunity to use a helpful characteristic, and medication administration failures that happen in the absence of such intentional design arise from “designer error” rather than “user error”. Guidelines that define a container’s shape for each class of medication would compel pharmaceutical manufacturers to be compatible and would eliminate the confusion that arises when a hospital changes the supplier of a given medication.
-
Content ArticleIn this blog, published by What's The Pont, the author provides a summary of the The Swiss Cheese Model of Accident Causation, developed by Professor James T. Reason, and looks at what it means for learning from failure. Related reading: The Swiss cheese respiratory virus pandemic defence Reverse Swiss Cheese – Driving safety culture from the blunt end (24 June 2022) Good and bad reasons: The Swiss cheese model and its critics (June 2020)
-
Content ArticleHealthcare relies on high levels of human performance; however, human performance varies and is recognised to fall in high-pressure situations, meaning that it is not a reliable method of ensuring safety. Other safety-critical industries embed human factors principles into all aspects of their organisations to improve safety and reduce reliance on exceptional human performance; there is potential to do the same in anaesthesia. This narrative review in the journal Anaesthesia aims to describe what is known about human factors in anaesthesia to date.
-
Content ArticleEurocontrol’s HindSight magazine is a magazine on human and organisational factors in operations, in air traffic management and beyond. This issue is on the theme of Handling Surprises: Tales of the Unexpected. You will find a diverse selection of articles from frontline staff, senior managers, and specialists in operations, human factors, safety, and resilience engineering in the context of aviation, healthcare, maritime and web operations. The articles reflect surprise handling by individuals, teams and organisations from the perspectives of personal experience, theory, research and training.
-
Content ArticleIt is difficult to monitor compliance to surgical checklists, which is associated with improved patient outcomes. This research study in The Annals of Surgery reported for the first time on the use of the Operating Room Black Box (ORBB) to track checklist compliance, engagement, and quality. The authors took a retrospective review of prospectively collected ORBB data and measures of checklist compliance, engagement and quality were assessed. ORBB provides the unprecedented ability to assess not only compliance with surgical safety checklists but also engagement and quality. This technology allows the assessment of compliance in near real time and to accurately address safety threats that may arise from noncompliance.
-
Content ArticleSafety-II is moving beyond the conceptual, with practical applications emerging from the fog of models and theory. But critics still point to a lack of evidence and limited real-world proof that the promise is justified. This blog reports on a webinar by Mark Sujan and Simon Gill that looked at how to implement Safety-II thinking in real world settings. The blog outlines different elements of the webinar including: a case study of anticipatory practice being used to reduce serious harm from falls in an emergency department a discussion on how to move towards a non-hierarchical clinical leadership challenges to adopting Safety-II principles evaluation of Safety-II: how do you measure a non-event?
-
Content ArticleIn this blog, Jonathan Back, Intelligence Analyst at the Healthcare Safety Investigation Branch (HSIB), looks at the opportunities the healthcare system has to adopt proactive risk management to improve patient safety. He highlights that understanding the value of different perspectives may provide new opportunities for improvement if applied across the health and care system. He also outlines the role of the new integrated care boards (ICBs) in achieving this whole-system approach, which should include a clinical governance perspective, organisational and local system perspective and societal perspective.
-
Content Article
 In a blog for National Voices, the leading coalition of health and social care charities in England, Patient Safety Learning’s Chief Executive Helen Hughes discusses an independent report written by risk expert Tim Edwards that highlights serious and widespread safety concerns around the misdiagnosis of pulmonary embolism.
In a blog for National Voices, the leading coalition of health and social care charities in England, Patient Safety Learning’s Chief Executive Helen Hughes discusses an independent report written by risk expert Tim Edwards that highlights serious and widespread safety concerns around the misdiagnosis of pulmonary embolism. -
Content Article
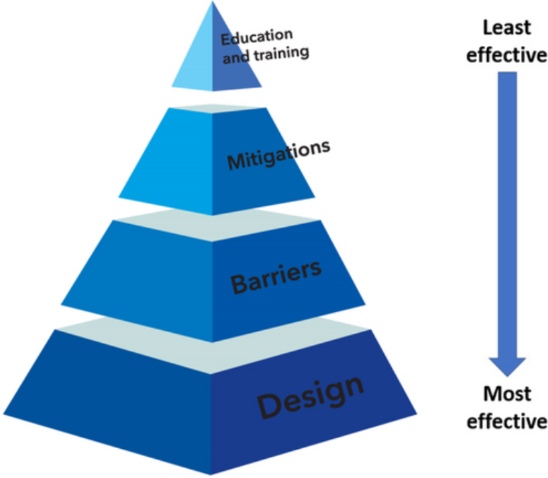 This guidance on implementing human factors in anaesthesia has been produced by the Difficult Airway Society and the Association of Anaesthetists. Human factors is an evidence-based scientific discipline used in safety critical industries to improve safety and worker wellbeing; implementing human factors strategies in anaesthesia has the potential to reduce the reliance on exceptional personal and team performance to provide safe and high-quality patient care. A three-stage Delphi process was used to formulate a set of 12 recommendations: these are described using a ‘hierarchy of controls’ model and classified into design, barriers, mitigations and education and training strategies.
This guidance on implementing human factors in anaesthesia has been produced by the Difficult Airway Society and the Association of Anaesthetists. Human factors is an evidence-based scientific discipline used in safety critical industries to improve safety and worker wellbeing; implementing human factors strategies in anaesthesia has the potential to reduce the reliance on exceptional personal and team performance to provide safe and high-quality patient care. A three-stage Delphi process was used to formulate a set of 12 recommendations: these are described using a ‘hierarchy of controls’ model and classified into design, barriers, mitigations and education and training strategies. -
Content ArticleIn this article, published by BMJ Opinion, author David Raven says: "Emergency care staff have been working under the shadow of a slow moving catastrophe for years". David, emergency medicine consultant and divisional director of urgent care, provides several examples of data and high level concerns raised that attempted to forewarn of these dangers. He argues that blaming Covid and high levels of flu for the pressures provides a false narrative to the reality and that the relentless hard work of staff is not enough to compensate for the challenges they face in what he says is a dysfunctional system.
-
Content ArticleThis BMJ Opinion piece is written by Chris Ham (in a personal capacity)who was chief executive of The King’s Fund from 2010 to 2018. Chris talks about the recent funding announcement to support hospital discharges in order to free up bed space. He highlights a number of key considerations including: the impact on patient involvement in their discharge decisions staff shortages in care homes bed capacity in care homes. Chris questions whether these decisions are 'symbolic policy making' or whether they will actually make a difference to patients.





