Search the hub
Showing results for tags 'Implementation'.
Found 186 results
-
Content ArticleOvercrowding in the emergency department (ED) is a global problem that causes patient harm and exhaustion for healthcare teams. Despite multiple strategies proposed to overcome overcrowding, the accumulation of patients lying in bed awaiting treatment or hospitalisation is often inevitable and a major obstacle to quality of care. This study in BMJ Open Quality looked at a quality improvement project that aimed to ensure that no patients were lying in bed awaiting care or referral outside a care area. Several plan–do–study–act (PDSA) cycles were tested and implemented to achieve and maintain the goal of having zero patients waiting for care outside the ED care area. The project team introduced and adapted five rules during these cycles: No patients lying down outside of a care unit Forward movement Examination room always available Team huddle An organisation overcrowding plan The researchers found that the PDSA strategy based on these five measures removed in-house obstacles to the internal flow of patients and helped avoid them being outside the care area. These measures are easily replicable by other management teams.
-
News ArticlePatients continue to experience avoidable harms from unsafe care because the NHS fails to learn from its mistakes, a report that tracked what actions the NHS took following safety reviews over several decades has found. Patient Safety Learning looked at the findings of a variety of investigations, including widespread public inquiries, Healthcare Safety Investigation Branch (HSIB) reports, Prevention of Future Deaths reports, incident reports, and complaints and legal action by patients and their families. It found an “implementation gap” in learning lessons and taking action to prevent future harms. It highlighted an absence of a systemic and joined up approach to safety; poor systems for sharing learning and acting on that learning; lack of system oversight, monitoring, and evaluation; and unclear patient safety leadership. Helen Hughes, chief executive of Patient Safety Learning, said, “Time and time again there is a lack of action and coordination in responding to recommendations, an absence of systems to share learning, and a lack of commitment to evaluate and monitor the effectiveness of safety recommendations. “This is a shocking conclusion that is an affront to all those patients and families who have been assured that ‘lessons have been learnt’ and ‘action will be taken to prevent future avoidable harm to others.’ The healthcare system needs to understand and tackle the barriers for implementing recommendations, not just continually repeat them.” The report calls for “systemwide commitment and resources, with effective and transparent performance monitoring” for patient safety inquiries and reviews and HSIB reports to ensure that the accepted recommendations translate into action and improvement. Read full story Source: BMJ, 8 April 2022
-
News Article
Bereaved call for body to enforce coroners’ advice

Patient Safety Learning posted a news article in News
Relatives of a teenage rape survivor who died after failures by mental health services are joining other families to demand a new body to enforce coroners’ recommendations to prevent future deaths. Campaigners claim the failure to act on hundreds of coroners’ recommendations every year, and to learn from the findings of often expensive inquiries into disasters, means the same mistakes are being repeated. Gaia Pope, 19, was diagnosed with post-traumatic stress disorder after revealing that she had been drugged and raped when she was 16. She was found dead in undergrowth on a cliff 11 days after disappearing in Swanage, Dorset, in 2017. After one of the longest inquests in legal history, the coroner, Rachael Griffin, made multiple reports last year to authorities including the NHS and police to prevent future deaths, but Pope’s family says most have not been acted upon. The Inquest campaign, which works with families bereaved by state-related deaths, is calling for a “national oversight mechanism” to collate recommendations and responses in a new national database, analyse responses from public bodies, follow up on progress and share common findings. Read full story (paywalled) Source: The Times, 27 June 2023 -
News Article
Update on LFPSE implementation deadline
Patient Safety Learning posted a news article in News
In an email to staff today (9 May 2023) NHS England (NHSE) have confirmed that to meet the deadline for implementing the new Learn From Patient Safety Events (LFPSE) service, Trusts will only need to ensure this is underway by the 30 September 2023, rather than fully implemented. LFPSE is a new central national service for recording and analysing patient safety events that occur in healthcare. Some NHS organisations are now using this system, instead of the National Reporting and Learning System (NRLS), and all organisations will be expected to transition to this. The original date for Trusts to implement LFPSE was the 31 March 2023. However, in response to concerns about the achievability of this deadline, on the 18 October NHSE announced an optional six-month extension, meaning that Trusts needed to deploy the new system by the 30 September 2023. Today’s email to NHS staff noted that some Trusts “are still anticipating challenges with the time scales”. Responding to this, NHSE clarified that provided the LFPSE transition within organisations Local Risk Management Systems was underway by the end of September, and that application of the guidance to configure formals and fields was being actively worked on, this milestone should be considered as having been met. Commenting on this Helen Hughes, Chief Executive of charity Patient Safety Learning, said: “This is a welcome announcement by NHS England, reducing the immediate pressure on staff who had raised serious concerns on the ability to have LFPSE configured and ready to submit events by the 30 September deadline. This flexibility will ensure that the new LFPSE service has a stronger chance of successful transition and to enable patient safety improvement”. -
Content ArticleJudy Walker talks about improving team performance through the After Action Review approach and the importance of AAR Conductor training.
-
Content ArticleThis download is the third of three chapters of a book which complements the Chartered Institute of Ergonomics and Human Factors' Healthcare Learning Pathway and is intended as a practical resource for students The book aims to provide well-founded, practical guidance to those responsible for leading and implementing human factors programmes and interventions in health and social care.
-
Content Article
Safety for All: 2022 Conference Report

Mark Hughes posted an article in Improving patient safety
This report provides an overview of speeches, presentations and panel sessions held at the inaugural Safety for All conference, which took place at the Royal College of Physicians in London on Wednesday 7 December 2022. It has been published by the Safety for All campaign, which calls for improvements in, and between, patient and healthcare worker safety to prevent patient safety incidents and deliver better outcomes for all. The campaign is supported by Patient Safety Learning and the Safer Healthcare and Biosafety Network. -
Content ArticleIntegrated care systems are now legally responsible for leading a localised approach that brings multiple aspects of the healthcare system closer together, and for working better with social care and other public services. However, this is not a new aspiration, so why should it be any different this time? The Nuffield Trust hosted a series of roundtables to discuss concerns with stakeholders and experts to try and understand how to ensure the aims are achieved. This report summarises these findings and offers ways forward as the new era gets underway.
-
Content ArticleThis article in BMJ Open Quality aimed to improve patient safety by examining the organisational and individual factors that contribute to adverse events, enabling corrective action so that errors are not repeated. Using interviews and observations of Trust meetings at a single Hospital Trust in the Midlands, England, this qualitative study: analysed whether the attitudes and behaviours of clinicians and managers are aligned with a Just Culture. identified barriers and enablers to an organisation adopting a Just Culture. The study found evidence of a fair incident management process within the Trust; however, there was no agreed vision of a Just Culture and the majority of the staff were unfamiliar with the term. Negative perspectives relating to clinical incidents and their management persist among staff with many having concerns about being the subject of an investigation and doubts about whether they drive improvement.
-
Content ArticleSafety-II is moving beyond the conceptual, with practical applications emerging from the fog of models and theory. But critics still point to a lack of evidence and limited real-world proof that the promise is justified. This blog reports on a webinar by Mark Sujan and Simon Gill that looked at how to implement Safety-II thinking in real world settings. The blog outlines different elements of the webinar including: a case study of anticipatory practice being used to reduce serious harm from falls in an emergency department a discussion on how to move towards a non-hierarchical clinical leadership challenges to adopting Safety-II principles evaluation of Safety-II: how do you measure a non-event?
-
Content ArticleIn this blog, Judy Walker, an After Action Review (AAR) expert, looks at how effective learning from disasters and incidents can restore hope and trust, offering long-term improvements to systems that have failed. She talks about how public inquiries, although they can seem frustratingly slow, benefit society when the relevant authorities ensure that learning is understood and implemented. She compares this to the impact of AARs, highlighting that people’s trust in the process is linked to their perception of the changes that happen as a result of the AAR. She outlines three steps that NHS providers should take to ensure the AAR process is effective in restoring hope: Highlight to all staff on a regular basis, the benefits that are being delivered due to AARs Ensure patients and family members are provided with specific information about how AARs prevent future harms Support the people who lead AARs to do so skilfully, so that quality is assured and staff can trust in the safety and value of the process.
-
Content Article
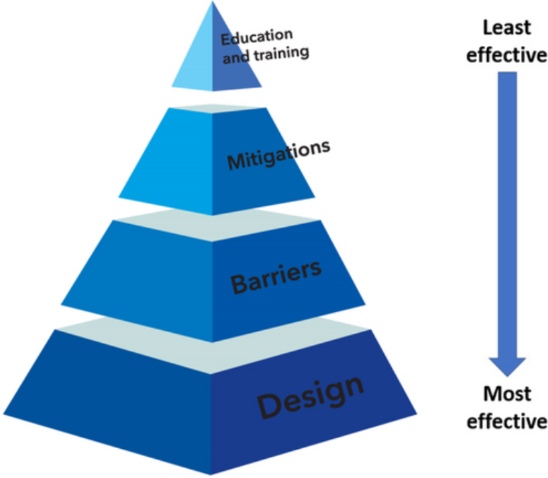 This guidance on implementing human factors in anaesthesia has been produced by the Difficult Airway Society and the Association of Anaesthetists. Human factors is an evidence-based scientific discipline used in safety critical industries to improve safety and worker wellbeing; implementing human factors strategies in anaesthesia has the potential to reduce the reliance on exceptional personal and team performance to provide safe and high-quality patient care. A three-stage Delphi process was used to formulate a set of 12 recommendations: these are described using a ‘hierarchy of controls’ model and classified into design, barriers, mitigations and education and training strategies.
This guidance on implementing human factors in anaesthesia has been produced by the Difficult Airway Society and the Association of Anaesthetists. Human factors is an evidence-based scientific discipline used in safety critical industries to improve safety and worker wellbeing; implementing human factors strategies in anaesthesia has the potential to reduce the reliance on exceptional personal and team performance to provide safe and high-quality patient care. A three-stage Delphi process was used to formulate a set of 12 recommendations: these are described using a ‘hierarchy of controls’ model and classified into design, barriers, mitigations and education and training strategies. -
Content ArticleThis document, Malaysian Patient Safety Goals 2.0 – Guidelines on Implementation & Surveillance explains the details of the new Malaysian Patient Safety Goals, known as MPSG 2.0. It describes the: Malaysian Patient Safety Goals and KPIs. The technical specifica!on of the associated KPIs (i.e., rationale, strategies & implementation, definition, inclusion and exclusion criteria, formula of KPI, numerator, denominator and target for each goal). The data collection process and format.
-
Content ArticleRecording of the Health and Social Care Committee meeting held on Tuesday 13 December 2022. Meeting started at 10.03am, ended 11.45am.
-
Content ArticleThis policy paper, published by the Department of Health and Social Care, provides an update on the UK Government’s progress in implementing the recommendations of the Independent Medicines and Medical Devices Safety (IMMDS) Review, sometimes referred to as the Cumberlege Review.
- Posted
- 3 comments
-
- (and 6 more)
-
Content ArticleIn this episode of the What the HealthTech? podcast, Radar Healthcare's Chief Product Officer Mark Fewster speaks to Helen Hughes, Chief Executive of Patient Safety Learning. to get the lowdown on NHS England's new Patient Safety Incident Response Framework (PSIRF). Helen talks about how PSIRF is going to drive an open and just culture, what can be expected after the transition and why the implementation process is key to PSIRF's success. Listen on Spotify Listen on YouTube
-
Content ArticleThis Canadian study in the Journal of Patient Safety describes an initiative that introduced system-wide changes to practice and patient safety culture in a rapid time frame. it looks at the implementation of a 'zero harm' approach to eliminate preventable harm across a wide variety of clinical areas. In less than a year, the intervention increased patient safety incident reporting by 37% while decreasing falls with injury by 39%, pressure injury rates by 37% and central line–associated blood stream infections by 34%.
-
Content Article
What is Appreciative Inquiry?
Patient Safety Learning posted an article in Improving patient safety
Appreciative Inquiry (AI) initiatives are implemented using the '4-D cycle' (Discovery, Dream, Design and Destiny). It's a methodology that allows an organisation to identify its positive core strengths relative to the 'affirmative topic' being addressed and and initiate concrete operational steps to achieve its goals. This article explains more. -
Content Article
 This is part of our series of Patient Safety Spotlight interviews, where we talk to people working for patient safety about their role and what motivates them. Beverley talks to us about setting up Thrombosis UK and how it has grown to have a national impact on patient safety in hospitals. She also describes the value of combining policy work with seeing patients face-to-face, and explores the need to find new ways of working to deal with the pressures facing the healthcare system.
This is part of our series of Patient Safety Spotlight interviews, where we talk to people working for patient safety about their role and what motivates them. Beverley talks to us about setting up Thrombosis UK and how it has grown to have a national impact on patient safety in hospitals. She also describes the value of combining policy work with seeing patients face-to-face, and explores the need to find new ways of working to deal with the pressures facing the healthcare system. -
Content ArticleThe objective of this study from Sharma et al. was to evaluate the accuracy of a new elective surgery clinical decision support system, the ‘Patient Tacking List’ (PTL) tool (C2-Ai(c)) through receiver operating characteristic (ROC) analysis. They found that the PTL tool was successfully integrated into existing data infrastructures, allowing real-time clinical decision support and a low barrier to implementation. ROC analysis demonstrated a high level of accuracy to predict the risk of mortality and complications after elective surgery. As such, it may be a valuable adjunct in prioritising patients on surgical waiting lists. Health systems, such as the NHS in England, must look at innovative methods to prioritise patients awaiting surgery in order to best use limited resources. Clinical decision support tools, such as the PTL tool, can improve prioritisation and thus positively impact clinical care and patient outcomes.
-
Content ArticleMinisters, high-level representatives and distinguished experts from all over the world gathered in Montreux on 23 and 24 February 2023 for the 5th Global Ministerial Summit on Patient Safety. They discussed achievements, challenges, priorities and necessary points of action. The summit marked another key milestone for global developments in patient safety. The Ministers and other participants reaffirmed that patient harm in health care is an urgent public health issue, pertinent to countries of all income settings and geographies and therefore a shared global challenge. Patient safety is essential for the achievement of universal health coverage and global health security. Read the Montreux Charter on Patient Safety launched at the Summit.
-
Content ArticleSometimes after an incident, a system-wide change is implemented that makes work more difficult and creates new problems. This story from aviation is one such example, which contains useful lessons for responding to rare events. Steven Shorrock recounts the tale.
-
Content ArticleImperial College Healthcare share a poster on their strategic goals and their values and behaviours.
-
Content ArticleThe number of patients who die from post-surgical complications in low- and middle-income countries is shockingly high. In Africa alone, more than 600,000 people die each year after surgery, mostly from causes that are relatively easy to treat. This blog by Pierre Barker, Chief Scientific Officer at the Institute for Healthcare Improvement (IHI) looks at a method for reducing post-surgical death called the '5Rs for rescue': Risk stratification Recognise deterioration Respond Reassess Reflect/Redesign He describes how the IHI will test how to support the reliable implementation of the '5Rs for Rescue', which aims to reduce mortality by 25%.
-
Content ArticleStatement from Maria Caulfield, Parliamentary Under Secretary of State (Minister for Mental Health and Women's Health Strategy) on the Government’s initial response to the report of the independent review into the maternity and neonatal services at East Kent University NHS Foundation Trust that was published on the 19 October 2022. NHS England commissioned Dr Bill Kirkup to undertake this review following concerns about the quality and outcomes of care.



